It’s Time for Us To Suspend Twitter for Spreading False and Misleading Information About the Safety of the C0VID Vaxxines
By Steve Kirsch
Twitter cancelled me for spreading false and misleading information. Here’s the original post I made about this and here’s the proof that my post was not misleading.
When I read through the posts on Twitter about the vaccines being safe and effective, it is very clear that it is Twitter that is spreading misinformation that is killing people.
But they aren’t holding themselves accountable for that. So it’s up to us.
I have decided to fund a massive ad campaign to encourage all Americans who believe in free speech to dump Twitter and switch to Gab, Telegram, and/or substack.
Step #1 is building a team with the talents to pull this off. Once we perfect this, we can replicate with the other platforms that censor the truth and allow false information to be spread.
If you want to help, please register here and check the “Twitter Switch Project” box.
If you have interest and expertise in this area, please register using this form (check the Twitter Switch Project box) and note any extra special skills at the end of the form.
Note: If you’ve already filled out the form, just edit it by adding the new checkbox.
Thanks!
As of Nov 26, we have 35 people interested in this project and over 400 people with various skills wanting to help out in other capacities.
Australian National Review is also launching its own campaign to encourage people to dump Fakebook, Instasham, Screwtube.
Powered by Australian National Review an independent, not-for-profit news media company, built by the people for the people, as well.
Also, the platform will be known as ANR Social too.
It will be censor-free and blockchain protected, it combines the best of YouTube Features for uploading videos, plus Telegram and Facebook-type features for ease of sharing articles or content and to keep in touch with family and friends privately and securely away from the eyes of the Government Agencies.
The Best C0VID Treatments for Hospitalized Patients
By Steve Kirsch
These methods below are proven to be effective, but they are not generally well known. None of them have ever caused a patient to worsen as far as we know, but physicians are generally unwilling to try any of them and will provide no justification for refusing to use them. If you want to use any of them, you will have to be very assertive and/or find a really good hospital and/or sue them.
In particular, you want to avoid two things like the plague. Both of these are generally a death sentence:
Remdesivir
Being put on a ventilator
I know of less than 5 hospitals in the US that would allow one or more of the treatments below. That is an indicator of how messed up our medical system is today since these are all “no brainers” if you take the time to look at each of them closely.
See which one(s) the doctor will support. You’ll want to get your own personal physician involved if he has hospital privileges. The doctor may get fired or lose privileges for authorizing any of these medications. It may be impossible for you to get them to the patient since you will be prohibited from seeing the patient even if you are vaccinated (since the hospital knows the vaccines don’t work).
Adenosine inhalation
ExThera Seraph 100
Flow Pharma FLOVID-20
Cyproheptadine
Cyclosporine
Fluxvoxamine or fluoxetine
Ivermectin
Proxalutamide
Fenofibrate
Vitamin D3
Aspirin
Inhaled Budesonide
Note: Leronlimab would have made the list, but the FDA hasn’t approved it, so it can only be used in clinical trials where it typically has more than an 85% success rate when used as directed. However, the FDA refused to allow the drug to be used for once a week for 4 weeks, so the trial results were unimpressive and the drug will not get an EUA.
Adenosine inhalation
Marked improvement in lung function observed in 5-10 minutes.
Treatment is 9mg adenosine in an inhaler given every 12 hours first day, then once a day for next 4 days.
93% survival rate; decreased time on vent, in ICU; lower viral load.
The mechanism of action seems to be a mix of effects on vasculature with inhibition of immune response, with the immune side being the most important.
The question was how to get FDA approval to use inhaled Adenosine for ultra rapid covid treatment due to the novel form of administration.
For more info, see the inhaled adenosine slide deck by Bruce Spiess. Clinical trial.
Adenosine paper: “Considering these hypotheses, a COVID-19 patient with unresponsive respiratory failure was treated with adenosine for compassionate use. The results showed a rapid improvement of clinical conditions, with negativity of SARS-CoV2 detection.”
ExThera Seraph 100
This device is a filter for your blood to extract out the virus. Basically, process is exactly like dialysis, but you use a special filter (the Seraph 100) on the dialysis machine. This filter will filters out SARS-CoV2 from your blood.
78% survival rate if given pre-vent. 100% survival rate if treated on day of or day after intubation. But the earlier you treat, the better the outcome.
Device cost is $1,500 per patient per time. Usually just one time (depends on viral load). Takes 4 hours to filter your blood.
800 patients, no problems in anyone.
Physicians normally make the mistake of waiting to use this until patients are on high flow oxygen because they are too conservative about the benefit/risk tradeoff, but it’s always better to use it earlier, e.g., as soon as someone has checked into the hospital. Patient is immediately better after 4 hours.
Works to both prevent and treat. Useful for long hauler too. Works across all coronaviruses. Best used early (right after infection) but can be used late stage.
Cyproheptadine
Cyproheptadine 8mg TID has proven to extricate patients from the ICU in 48 hours repeatedly. Doesn’t work a small percentage of patients, but never does harm. There will be a clinical trial to prove this works soon. Dr. Farid Jalali and Dr. Philippe Rola discovered this. There is a paper to back this up and case studies, but both are not published yet.
For anyone with oxygen requirements and covid, cyproheptadine will benefit them. If early disease without o2 requirements, fluvoxamine is the way to go.. Basically, if you didn’t get fluvoxamine early (which would have kept platelets from getting loaded up with serotonin), then your platelets will release that serotonin when the virus attacks. This means its too late for fluvoxamine to undo that damage (the genie is out of the bottle already), so cyproheptadine blocks the receptors that serotonin would otherwise activate. So basically fluvoxamine keeps the horses from leaving the stable, but once the horses have left the stable, then you use the cyproheptadine to keep the horses from doing any damage.
For better results combine with Famotidine 40 mg BID
See my tweet on cyproheptadine for more info.
Cyclosporine
Hooman Noorchashm is the champion of this approach used for late stage COVID patients. See his Medium article on cyclosporine.
10/10 success record per patients enrolled using this protocol.
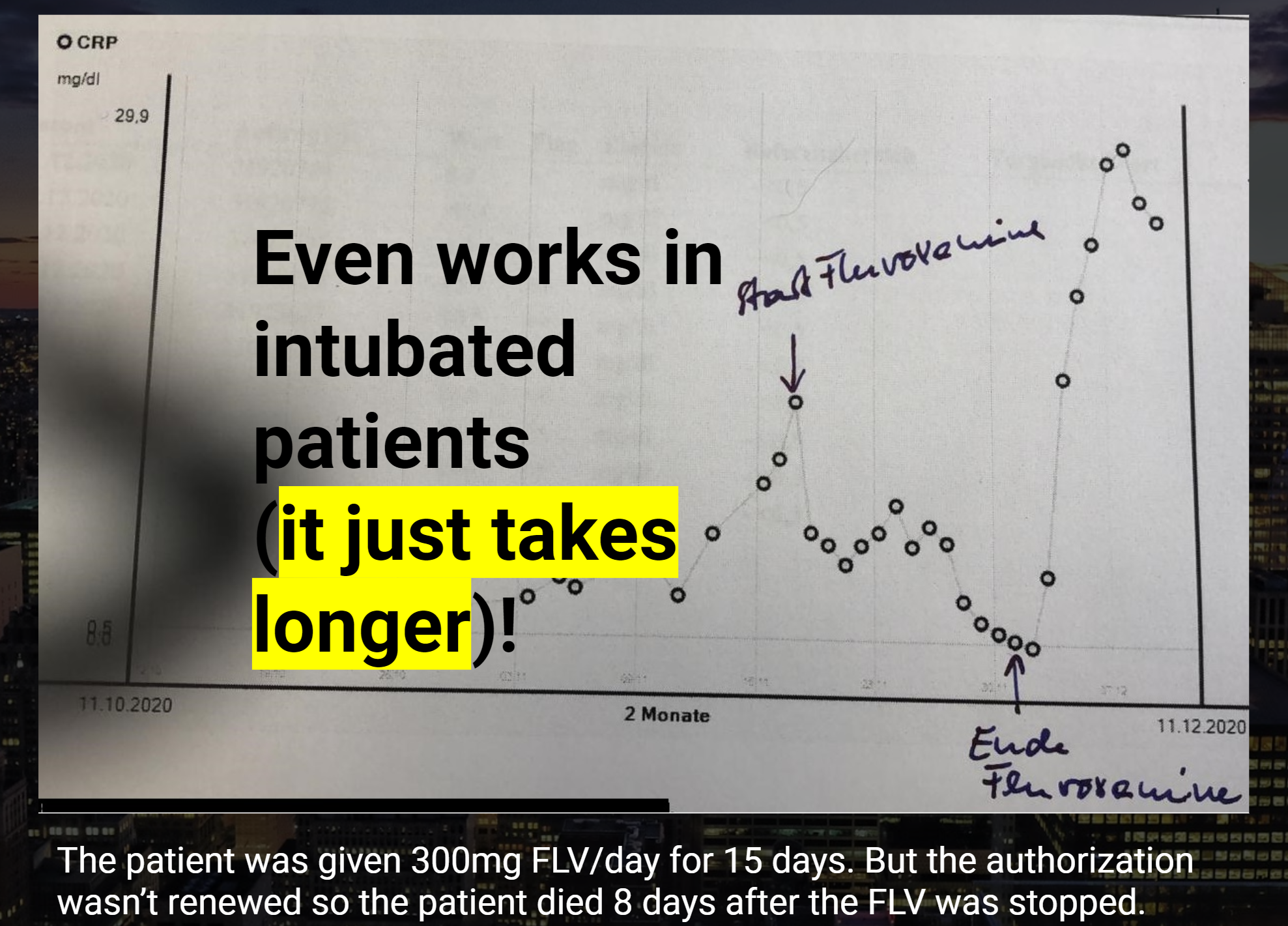
Fluxvoxamine
100mg TID of fluvoxamine can salvage patients and the effects are almost instant:
Fenofibrate
This drug is a no brainer for hospitalized patients due to respiratory distress since there are no downsides, the drug is cheap, and it works rapidly to relieve respiratory distress. 145mg/day for 10 days. There is a trial in the US for hospitalized patients on this drug.
Proxalutamide
Proven in large RCT to reduce death rate by 92% for hospitalized patients. It’s a pill. Available only in clinical trial, but should be available via Right to Try because there is an active IND at the FDA as of March 5, 2021.
For details, see this presentation or read this article or this article.
There is also an outpatient trial with superb results.
Ivermectin
A very safe drug that can cut your risk of dying in half. Has worked even for patients who are close to dying.
Vitamin D3
This reduces your risk even if you are sufficient in Vitamin D3. It is surprisingly more effective than you’d guess. A factor of 2 or more could be the difference between life and death.
One of the most commonly used tricks to make a drug look more effective than it is in a real-world setting is to conflate absolute and relative risk reduction. While AstraZeneca boasted a relative reduction of 100%, the absolute reduction was 0.01%. For the Pfizer shot, the relative risk reduction was initially 95%, but the absolute risk reduction was only 0.84%
In AstraZeneca’s trial, only 0.04% of people in the vaccine group, and 0.88% in the placebo group were infected with SARS-CoV-2. When the background risk of infection is that low, even a 100% absolute risk reduction becomes near-meaningless
Research shows the majority of SARS-CoV-2-specific antibodies in obese COVID-19 patients are autoimmune and not neutralizing. This means that if you’re obese, you’re at risk of developing autoimmune problems if you get the natural infection. You’re also at higher risk of a serious infection, as the antibodies your body produces are not the neutralizing kind that kill the virus. Does the same hold true for antibodies made in response to the COVID jab?
At nearly 72%, Vermont has the highest rate of “fully vaccinated” residents in the country, yet COVID cases are suddenly surging to new heights. During the first week of November 2021, cases increased by 42%. The hospital admission rate for fully vaccinated patients increased by 8%, while the admission rate for those who were not fully vaccinated decreased by 15%. Local health authorities blame the surge on the highly infectious delta variant, which would be odd if true, since the first delta case in Vermont was detected back in mid-May
Data from physician assistant Deborah Conrad show vaccinated people — counting anyone who got one or more shots, regardless of time since the injection — are nine times more likely to be hospitalized than the unvaccinated
In a November 12, 2021, blog post,1 Maryanne Demasi, Ph.D., reviews how the benefits of the COVID-19 shots have been exaggerated by the drug companies and misrepresented to the public by an uncritical media. She has previously given many lectures on how the drug companies conflated absolute and relative risks for statin drugs.2
Demasi was a respected Australian science presenter at ABC television until she produced a Catalyst report on the dangers of Wi-Fi and cellphones. In the wake of the controversy it raised, she and 11 of her staff members were axed and the episode retracted.3 That was 2016. Today, Demasi is one of the few professional journalists seeking and publishing the truth about COVID-19.
Absolute Versus Relative Risk Reduction
In her post, Demasi highlights one of the most commonly used tricks in the book — conflating absolute and relative risk reduction. As noted by Demasi, AstraZeneca and Australia’s health minister, Greg Hunt, claimed the AstraZeneca injection offered “100% protection” against COVID-19 death. How did they get this number? Demasi explains:4
“In the trial5 of 23,848 subjects … there was one death in the placebo group and no deaths in the vaccinated group. One less death out of a total of one, indeed was a relative reduction of 100%, but the absolute reduction was 0.01%.”
Similarly, Pfizer’s COVID shot was said to be 95% effective against the infection, but this too is the relative risk reduction, not the absolute reduction. The absolute risk reduction for Pfizer’s shot was a meager 0.84%.
It’s worth noting that an incredibly low number of people were infected in the first place. Only 8 out of 18,198 vaccine recipients developed COVID symptoms (0.04%), and 162 of the 18,325 in the placebo group (0.88%).
Since your risk of COVID was minuscule to begin with, even if the shot was able to reduce your absolute risk by 100%, it would still be trivial in real-world terms.
According to Gerd Gigerenzer, director of the Harding Centre for Risk Literacy at the Max Planck Institute, only quoting the relative risk reduction is a “sin” against transparent communication, as it can be used as a “deliberate tactic to manipulate or persuade people.” Demasi also quotes John Ioannidis, professor at Stanford University, who told her:6
“This is not happening just for vaccines. Over many decades, RRR [relative risk reduction] has been the dominant way of communicating results of clinical trials. Almost always, RRR looks nicer than absolute risk reductions.”
Demasi continues:7
“When asked if there was any justification for misleading the public about the vaccine’s benefits to encourage uptake, Prof Ioannidis rejected the notion.
‘I don’t see how one can increase uptake by using misleading information. I am all in favor of increasing uptake, but this needs to use complete information, otherwise sooner or later incomplete information will lead to misunderstandings and will backfire,’ says Ioannidis.
The way authorities have communicated risk to the public, is likely to have misled and distorted the public’s perception of the vaccine’s benefit and underplayed the harms. This, in essence, is a violation of the ethical and legal obligations of informed consent.”
US Health Authorities Have Misrepresented the Data
U.S. health authorities, like Australia’s, are guilty of misrepresenting the data to the public. In February 2021, Centers for Disease Control and Prevention director Rochelle Walensky co-wrote a JAMA paper8 which stated that “Clinical trials have shown that the vaccines authorized for use in the U.S. are highly effective against COVID-19 infection, severe illness and death.”
Alas, “there were too few deaths recorded in the controlled trials at the time to arrive at such a conclusion,” Demasi writes.9 This observation was made by professor Peter Doshi, associate editor of The BMJ, during Sen. Ron Johnson’s Expert Panel on Federal Vaccine Mandates, November 1, 2021.10 During that roundtable discussion, Doshi stated that:
“The trials did not show a reduction in deaths, even for COVID deaths … Those who claimed the trials showed that the vaccines were highly effective in saving lives were wrong. The trials did not demonstrate this.”
Indeed, the six-month follow-up of Pfizer’s trial showed 15 deaths in the vaccine group and 14 deaths in the placebo group. Then, during the open label phase, after Pfizer decided to eliminate the placebo group by offering the actual shot to everyone who wanted it, another five deaths occurred in the vaccine group.
Two of those five had originally been in the placebo group, and had taken the shot in the open label phase. So, in the end, what we have are 20 deaths in the vaccine group, compared to 14 in the placebo group. We also have the suspicious fact that two of the placebo participants suddenly died after getting the real deal.
How You Express Effect Size Matters
As noted in a July 2021 Lancet paper,11 “fully understanding the efficacy and effectiveness of vaccines is less straightforward than it might seem. Depending on how the effect size is expressed, a quite different picture might emerge.”
The authors point out that the relative risk reduction really needs to “be seen against the background risk of being infected and becoming ill with COVID-19, which varies between populations and over time.” This is why the absolute risk reduction figure is so important:12
“Although the RRR considers only participants who could benefit from the vaccine, the absolute risk reduction (ARR), which is the difference between attack rates with and without a vaccine, considers the whole population …
ARR is also used to derive an estimate of vaccine effectiveness, which is the number needed to vaccinate (NNV) to prevent one more case of COVID-19 as 1/ARR. NNVs bring a different perspective: 81 for the Moderna–NIH, 78 for the AstraZeneca–Oxford … 84 for the J&J, and 119 for the Pfizer–BioNTech vaccines.
The explanation lies in the combination of vaccine efficacy and different background risks of COVID-19 across studies: 0.9% for the Pfizer–BioNTech … 1.4% for the Moderna–NIH, 1.8% for the J&J, and 1.9% for the AstraZeneca–Oxford vaccines.
ARR (and NNV) are sensitive to background risk — the higher the risk, the higher the effectiveness — as exemplified by the analyses of the J&J’s vaccine on centrally confirmed cases compared with all cases: both the numerator and denominator change, RRR does not change (66–67%), but the one-third increase in attack rates in the unvaccinated group (from 1.8% to 2.4%) translates in a one-fourth decrease in NNV (from 84 to 64) …
With the use of only RRRs, and omitting ARRs, reporting bias is introduced, which affects the interpretation of vaccine efficacy.
When communicating about vaccine efficacy, especially for public health decisions such as choosing the type of vaccines to purchase and deploy, having a full picture of what the data actually show is important, and ensuring comparisons are based on the combined evidence that puts vaccine trial results in context and not just looking at one summary measure, is also important.”
The authors go on to stress that comparing the effectiveness of the COVID shots is further hampered by the fact that they use a variety of different study protocols, including different placebos. They even differ in their primary endpoint, i.e., what they consider a COVID case, and how and when diagnosis is made, and more.
“We are left with the unanswered question as to whether a vaccine with a given efficacy in the study population will have the same efficacy in another population with different levels of background risk of COVID-19,” the authors note.
One of the best real-world examples of this is Israel, where the relative risk reduction was 94% at the outset and an absolute risk reduction of 0.46%, which translates into an NNV of 217. In the Phase 3 Pfizer trial, the absolute risk reduction was 0.84% and the NNV 119.13 As noted by the authors:14
“This means in a real-life setting, 1.8 times more subjects might need to be vaccinated to prevent one more case of COVID-19 than predicted in the corresponding clinical trial.”
SARS-CoV-2 Specific Antibodies Pose Danger for the Obese
In related news, a recent study15 published in the International Journal of Obesity warns that “the majority of SARS-CoV-2-specific antibodies in COVID-19 patients with obesity are autoimmune and not neutralizing.”
In plain English, if you’re obese, you’re at risk of developing autoimmune problems if you get the natural infection. You’re also at higher risk of a serious infection, as the antibodies your body produces are not the neutralizing kind that kill the virus. As explained by the authors:16
“SARS-CoV-2 infection induces neutralizing antibodies in all lean but only in few obese COVID-19 patients. SARS-CoV-2 infection also induces anti-MDA [malondialdehyde, a marker of oxidative stress and lipid peroxidation] and anti-AD [adipocyte-derived protein antigens] autoimmune antibodies more in lean than in obese patients as compared to uninfected controls.
Serum levels of these autoimmune antibodies, however, are always higher in obese versus lean COVID-19 patients. Moreover … we also evaluated the association of anti-MDA and anti-AD antibodies with serum CRP and found a positive association between CRP and autoimmune antibodies.
Our results highlight the importance of evaluating the quality of the antibody response in COVID-19 patients with obesity, particularly the presence of autoimmune antibodies, and identify biomarkers of self-tolerance breakdown. This is crucial to protect this vulnerable population at higher risk of responding poorly to infection with SARS-CoV-2 than lean controls.”
Now, these findings apply to obese people who develop the natural infection, but it makes one wonder whether the same holds true for the COVID jab. If the antibodies produced in response to the actual virus are primarily autoantibodies, will obese people develop autoantibodies instead of neutralizing antibodies in response to the COVID shot as well?
For clarity, an autoantibody is an antibody that is directed against one or more of your own body’s proteins. Many autoimmune diseases are caused by autoantibodies that target and attack your own tissues or organs.
So, this is no small concern, seeing how the mRNA in the COVID shots (and subsequent SARS-CoV-2 spike protein, which is what your body produces antibodies against) gets distributed throughout your body and accumulates in various organs.17,18
At this point, there’s an overwhelming amount of evidence showing the COVID shots are not working. What little protection you do get clearly wanes within a handful of months, and may leave you worse off than you were before. We’re seeing data to this effect from a number of different places.
In the U.S., we can now look at Vermont.19 At nearly 72% vaccinated, it has the highest rate of “fully vaccinated” residents in the country, according to ABC News,20 yet COVID cases are now suddenly surging to new heights.
U.S. Centers for Disease Control and Prevention data show Vermont had the 12th highest COVID case rate in the nation as of November 9, 2021. Over the previous seven days, cases had increased by 42%. It couldn’t have been due to a surge in testing, though, as the weekly average of tests administered had only increased by 9% in that time.
What’s more, during that first week of November, the hospital admission rate for patients who were fully vaccinated increased by 8%, while the admission rate for those who were not fully vaccinated actually decreased by 15%.
Keep in mind that you’re not considered “fully vaccinated” until two weeks after your second injection. If you got your second dose a week ago and end up in the hospital with COVID symptoms, you’re counted as unvaccinated. This gross manipulation of reality makes it very difficult to interpret the data, but even with this manipulation it is beyond obvious that the vaccines are failing.
Overall, the case rate in Vermont is FAR higher now than it as in the fall of 2020, when no one had gotten the “vaccine.” According to Vermont health commissioner Dr. Mark Levine, the surge is occurring primarily among unvaccinated people in their 20s and children aged 5 through 11 — a curious coincidence, seeing how the shots are just now being rolled out for 5- to 11-year-olds.
Levine blames the surge on the highly infectious delta variant, but delta has been around for months already. The first case of delta in Vermont was identified in mid-May 2021.21 Surely, it wouldn’t have taken six months for this most-infectious of variants to make the rounds and cause an unprecedented spike?
Two clues are given by Levine, however, when he admits that a) Vermont has one of the lowest rates of natural immunity in the U.S. and b) protection is waning among those who got the COVID shot early to mid-year. Breakthrough cases among the fully vaccinated shot up 31% during the first week of November.22
Fully Vaxxed Are Nine Times More Likely To Be Hospitalized
Coincidentally, data from physician assistant Deborah Conrad, presented by attorney Aaron Siri23 October 17, 2021, shows vaccinated people are nine times more likely to be hospitalized than the unvaccinated.
The key, however, was in what they counted as vaccinated. Rather than only including those who had gotten the shot two weeks or more before being hospitalized, they simply counted those who had one or more shots, regardless of when, as vaccinated. This gives us an honest accounting, finally! As explained by Siri:24
“A concerned Physician Assistant, Deborah Conrad, convinced her hospital to carefully track the COVID-19 vaccination status of every patient admitted to her hospital. The result is shocking.
As Ms. Conrad has detailed, her hospital serves a community in which less than 50% of the individuals were vaccinated for COVID-19 but yet, during the same time period, approximately 90% of the individuals admitted to her hospital were documented to have received this vaccine.
These patients were admitted for a variety of reasons, including but not limited to COVID-19 infections. Even more troubling is that there were many individuals who were young, many who presented with unusual or unexpected health events, and many who were admitted months after vaccination.”
Despite these troubling findings, health authorities ignored Conrad when she reached out. In mid-July 2021, Siri’s law firm also sent formal letters to the CDC, the Health and Human Services Department and the U.S. Food and Drug Administration on Conrad’s behalf,25 and those were ignored as well.
“This again highlights the importance of never permitting government coercion and mandates when it comes to medical procedures,” Siri writes.26
Now, one of the most shocking details gleaned from Conrad’s data collection, which Siri failed to make clear but Steve Kirsch highlights in a recent substack post is that:27
“The only way you can get those numbers is if vaccinated people are 9 times more likely to be hospitalized than unvaccinated. It is mathematically impossible to get to those numbers any other way. Period. Full stop. This is known as an ‘inconvenient truth.’”
Indeed, the more data we gain access to, the worse it looks for these COVID shots. Unfortunately, those who push them seem hell-bent on ignoring any and all data that don’t support their stance.
Worse, it seems data and statistics are being intentionally manipulated by our health authorities to present a false picture of safety and effectiveness. All such tactics are indefensible at this point, and people who believe the official narrative without doing their own research do so at their own risk.
How Your Vaxxination Status Will Only Be Temporary
By Dr. Joseph Mercola
Data suggest 1 in 317 boys aged 16 to 17 will get myocarditis from the COVID shots, and after a third booster, that number may be even higher
VAERS reporting is likely underreported by a factor of 41. Since there are over 8,000 domestic deaths reported to VAERS, and 98% of those deaths are “excess deaths,” this suggests that as many as 300,000 Americans may have died from the COVID shots thus far
Calculations based on government data from 35% of the world’s population suggest we’re killing approximately 411 people per million doses on average. Moderna and Pfizer are both two-dose regimens, which pushes this to 822 deaths per million fully vaccinated. And that’s just the short-term mortality. We still have no concept of how these shots might impact mortality and morbidity in the longer term
An Italian investigation found that if the COVID mortality definition were changed to only include those cases where there were no preexisting comorbidities, the mortality from COVID comes out to just 2.9% of the overall reported number. This suggests that if a COVID death was redefined to being a death actually “from” COVID rather than “with” COVID, the death count could be substantially smaller than 760,000 deaths and may be smaller than the number killed by the vaccines
The deadliest vaccine ever made is the smallpox vaccine, which killed 1 in 1 million vaccinated people. The COVID shots kills 822 per million fully vaccinated, making it more than 800 times deadlier than the deadliest vaccine in human history
In this interview, Steve Kirsch, executive director of the COVID-19 Early Treatment Fund, reviews some of the COVID jab data he’s presented to the U.S. Food and Drug Administration and the Centers for Disease Control and Prevention during various meetings.
For example, during the September 17, 2021, FDA VRBPAC (Vaccines and Related Biological Products Advisory Committee) meeting,1 Kirsch cited data suggesting 1 in 317 boys aged 16 to 17 will get myocarditis from the shots, and after a third booster, that number may be even higher. He also cited data showing the Pfizer shot kills far more people than it saves. I’ll provide more details about that below.
Kirsch didn’t come into this due to some preconceived opinion about vaccines. He and his family have all received two doses of the COVID jab. It wasn’t until after the fact that he started hearing about problems from others that he started taking deep dives into the data. He explains:
“After I got vaccinated, a woman asked me, ‘Should I get vaccinated?’ And I said, ‘Of course, you should. This is the safest thing ever. Nobody’s died and there are no side effects. You’ve got to get this modern technology.’ I’m singing from the hymn book.
And then she said something that threw me off course because I said, ‘Why are you asking such a stupid question?’ And she said, ‘Well, three of my relatives got the vaccine and they died within a week.’ I said, ‘No, no, that can’t be true. There’s no way that can happen.’
I’m trying to convince her that she’s mistaken, that it must have been something else. I wrote her saying, ‘Statistically, you can’t have three people dying from the vaccine, which doesn’t kill anyone.’ And she wrote back and she said, ‘Yeah, but they’re dead.’
That was a game-changing moment for me … but I was still in denial … I was operating [from the position] that the FDA is still operating the same [conservative] way [they used to before], but they’re not … nor did I understand that the U.S. Centers for Disease Control and Prevention is now mission driven, and the mission is to get a needle in every arm. My trust was in the agencies.
The next incident involved my carpet cleaner, Tim Damroth. He showed up wearing a mask. And I’m saying, ‘Hey, you should all get vaccinated. Once you get vaccinated you don’t have to wear a mask.’ And he said, ‘Well, I did get vaccinated, but I had an extreme reaction. I had a heart attack two minutes after I got injected.’ He also described that his wife had [developed] Parkinson’s-like symptoms. Her left hand was shaking uncontrollably.”
The Price Truth-Tellers Pay
The data are ultimately what convinced him that people must be told the truth about these shots because, without that, they cannot give informed consent. He’s sacrificed a lot to do just that, including professional relationships and millions of dollars in lost income.
“I basically put my life on hold and started looking in the various databases and talking to people to understand what was going on,” Kirsch says. “And every place I looked, [the truth] became more clear to me. And so, on May 25, 2021, I wrote this 250-page article for TrialSiteNews. It may be the longest article for TrialSiteNews ever published.
When I wrote that article, within a week, every member of my [COVID-19 Early Treatment Fund’s] scientific advisory board quit — there were 14 scientists from all over the United States and in different fields with different expertise. They said I was ‘an evil person’ and that they never wanted to talk to me again in their life.
I pleaded with them, saying, ‘Look, if I’ve got the analysis wrong, then tell why can’t you tell me where I got it wrong.’ And they wouldn’t say anything. They just said, the vaccines are safe and I should be ashamed of myself.”
Kirsch also created and submitted a 177-page PDF slideshow to the October 26, 2021, VRBPAC hearing, titled, “Questions About the COVID Vaccine.”2 It’s an absolute treasure trove of information and I would encourage you to review this great resource that he is updating in real time.
VAERS Data Likely Off by Factor of 41
In his video, “Vaccine Secrets: COVID Crisis,”3 the first episode of “The False Narrative Takedown Series,” Kirsch explains how to estimate COVID jab mortality, which he and a team of statisticians have done based on a variety of sources, including but not limited to the U.S. Vaccine Adverse Events Reporting System (VAERS).
Kirsch estimates VAERS reporting is off by a factor of 41, and that anywhere from 150,000 to 300,000 Americans have died from the COVID shots.
“We looked at eight different ways and VAERS is just one of the ways. So, when people say, ‘You can’t use VAERS for this, you can’t [calculate] causality [based on VAERS data], I’m saying, ‘Fine. We got the same answer using seven other ways.
In the VAERS analysis, we determined that VAERS was under-reported by a factor of 41, which is quite reasonable … Ten years ago we had a system where we could actually discover all the unreported things in VAERS, and they discovered VAERS was severely underreported by as much as 95 times. Vaccines that we thought were safe, they’re not safe at all. So, what did they do? They killed the project.
So, the reason that we have such a bad system today is that it is intentional. If we had a good system, it would show all the flaws for all of these vaccines that we’ve been giving people.”
The system is clearly intentionally designed from a technical standpoint to radically decrease the number of cases entered. It takes more than 30 minutes to complete a single report and you can’t save it until completed, so if you walk away and get timed-out, you have to start all over.
Kirsch knows a neurologist in California who claims to have 2,000 COVID jab-injured patients (out of a client base of 20,000), but she’s only filed two reports to VAERS. She doesn’t have time for the rest. So, she’s under-reporting by a factor of 1,000. Also, while doctors are required by law to file adverse event reports, there’s no enforcement, and no punishment for not filing.
It is also important to note that no one is paid to enter this data. That could be a part time job for most clinicians, were they to responsibly report all the side effects and deaths.
COVID Shots Are Far Deadlier Than the Infection
Overall, his team’s calculations suggest we’re killing 411 people per million doses (and remember Moderna and Pfizer are both two-dose regimens), worldwide. And that’s just the short-term mortality. We still have no concept of how these shots might impact mortality in the longer term.
To put things into further perspective, October 21, 2021, an Italian investigation found that by changing the COVID mortality definition to only include cases where COVID-19 was the primary cause of death and there were no comorbidities decreased the death toll by 97%, from 130,000 to fewer than 4,000.
Kirsch believes the real death tally from COVID-19 in the U.S. may be about 50% of the reported number. This means about 380,000 Americans died from COVID-19 (rather than with COVID), whereas the COVID “vaccine” has killed as many as 300,000. In other words, it’s possible that the cure may be worse than the disease.
COVID Shot Is the Deadliest ‘Vaccine’ Ever Created
It gets even worse though. In Pfizer’s children’s trial, one of the participants, 12-year-old Maddie De Garay, suffered a number of devastating events, including paralysis. This side effect was misreported, however, and put down as “abdominal pain.” Neither the FDA nor the CDC has investigated the case, despite promising to do so. Pfizer has refused to investigate it as well.
In the youth trial, 1 out of 1,131 children was paralyzed. Meanwhile, Pfizer’s adult trial shows that the shot saves one COVID death for every 22,000 fully-vaccinated people. But for children, it’s estimated we need to fully vaccinate over 630,000 kids to save one life. That means we may permanently disable as many as 557 kids per life saved. Meanwhile, there’s not a single report of a healthy child dying from SARS-CoV-2 infection anywhere in the world.
This means the number needed to vaccinate to save one otherwise healthy child from COVID death is actually infinite, as they’re not dying from COVID to begin with. There simply is no doubt that in children, the COVID shot is no benefit and all risk. Kirsch notes:
“Dr. Paul Offit was interviewed 20 years ago on ‘CBS 60 Minutes,’ and he said the smallpox vaccine is so dangerous that we would never consider doing that in modern times. It’s the most dangerous vaccine ever invented … and the smallpox vaccines only kills one person per every million-people vaccinated, which is a lot.
You vaccinate 300 million people, you’re going to kill 300 people. That is unacceptable according to Offit, but he just voted for a vaccine that kills 822 people per million fully vaccinated [assuming a two-dose regimen].
That means these COVID vaccines are over 800 times deadlier than the deadliest vaccine in human history. So, this isn’t a close call. These vaccines are the deadliest vaccines ever created by man. And they’re promoted as safe and effective.”
COVID Shot Gets Deadlier the Younger You Are
Based on a request from Dr. Peter McCullough, Kirsch also analyzed COVID jab mortality based on age using the VAERS data. For 80-year-olds, he found we kill two people to save one. For 20-year-olds, we kill six to save one.
The younger you are, the greater the risk. The Kostoff analysis4 found this general pattern as well. Ronald N. Kostoff is a research affiliate in Gainesville, Virginia, who in 2016 wrote an expert review on under-reporting of adverse events in the biomedical literature.5
In a review published in October 2021, Kostoff found five elderly are killed by the shots for each elderly person saved, and the ratios get worse as you go down in age. That said, “the vaccines don’t make sense for any age group, which is exactly the same thing I found independently,” Kirsch says.
“Nobody should get these vaccines. There is no cost-benefit analysis that I have seen that shows it is beneficial … I mean, you’re not going to take an intervention that is just as likely to kill you as to save you.
You want to take an intervention which is at least 10 times more likely to save you than to kill you, because it’s an optional intervention. What kind of business do you have taking an intervention which has a marginal benefit for a completely unknown short- and long-term risk profile?
The other thing I want to say is that, the societal benefit argument, people are saying, ‘You’re selfish because you didn’t get vaccinated.’ Well, that’s irrational.
Have you ever seen a CDC analysis showing you the societal benefit of being vaccinated? It doesn’t exist. And there’s a reason it doesn’t exist, because the societal benefit would be so tiny that it’s ludicrous. Today, we know the vaccinated are as likely to spread the virus as the unvaccinated. So where is the societal benefit?
If there are no downsides [to the shot], then people would say, sure, maybe there’s some societal benefit. I’ll do that. But here your life is at stake and the data show that roughly 1 in 1,000 will get killed by these vaccines. So, if I say, hey, suppose sacrificing your life could save 100 person years (e.g., 10 people given another 10 years of life).
When I asked this live in a clubhouse room with a few hundred people, nobody raised their hand to volunteer to do that — to sacrifice their life to save 100 person years. And I said, ‘OK, what about 1,000 person years? If you could sacrifice your life to save people 1,000 person years, would you do it? Nobody would do that. It’s nonsensical.
We have a constitutional right to life … And I don’t think you’re being selfish about it. You have a family, you have friends, you have loved ones, you have people you interact with … Why would I ask you to sacrifice your life? To save people you don’t know?
Everybody has their own special way that they contribute to society. Why would we ever ask somebody to [sacrifice their life for a potential social benefit]? Maybe we should ask Joe Biden, ‘Joe, if you could give up your life to save 1,000 person-years, would you do that?’ It would be very interesting to see what he says.”
CDC Performs Statistical Magic, Again
Countering all of this data we have a recent CDC analysis,6 which concluded that people who get the COVID shot are two-thirds less likely to die of any cause.
“I sent Janet Woodcock my deck of 180 questions. I said, ‘Janet, I bet you can’t answer any of these 180 questions. Doesn’t this concern you?’ She sends back an email saying, ‘Look at the CDC analysis, showing that after you get the jab, there’s this two-thirds drop in mortality.’
My friends and I, when we saw in that paper, we were laughing our heads off over here. The stats on 18- to 44-year-olds [show] 35% die from accidents. The rest die from disease — cancer, heart disease, whatever.
The only way to get a two-thirds reduction [in all-cause mortality] is if nobody dies from anything anymore — any disease — and we also reduce the number of accidents that they have … This is the immortality drug. All kidding aside, there’s no mechanism of action that could possibly justify that people are going to be better off from a health perspective after getting these vaccinations. Zero.
Nothing is improved. You are not immortal. You are just the opposite; your immune system is compromised. You’re also more likely to get COVID. In the U.K., the government numbers show that 40-year-olds, after the honeymoon period is over, were more than twice as likely to get infected if they were vaccinated.
In the U.S., you have hospitals where you have a 50% community vaccination rate and the hospital admissions are 90% vaccinated people. You can’t make these statistics up.
In fact, the CDC was confronted by these statistics by Aaron Siri, who wrote about it on his substack, and they just ignored them. So, they make up stuff [and] this paper shows the CDC can put out anything and as long as it has that little CDC logo on it, people are going to believe it no matter how ridiculous it is.
And nobody in the medical community criticized it. I wrote a very popular article about it on my substack entitled, ‘FDA Discovers Fountain of Youth.’”
Biggest Fraud in History
All things considered, the COVID vaccination campaign is the biggest medical fraud in modern history. As Kirsch says, it’s a house of cards, held together by belief in data that aren’t there and avoidance of confronting the safety signals in the VAERS system and other studies that don’t comport with the narrative.
They even avoided the determination of one of the world’s top pathologists (Peter Schirmacher) that at least 30% to 40% of the deaths two weeks post-vaccine were caused by the vaccine. The still claim there are no deaths that have been attributed to the Pfizer or Moderna vaccines. That’s ridiculous.
“I’ve never seen anything like this, and I’ve never heard of anything like this because the conspirators who are telling this false narrative are all the three-letter agencies under the Department of Health and Human Services — the FDA, CDC and NIH.
They’re all in on it, Congress is all in on it, mainstream media’s all in on it, and the medical community is all in on it. They can’t afford to back down now because they are in it too deep. It would be too embarrassing to them.
We have been saying for months, ‘You guys have to look at the VAERS data,’ and they have been ignoring and censoring us rather than engaging us with dialogue — and none of these people will engage us in dialogue.
We tell the so-called ‘fact checkers’ where to look and what questions to ask the CDC to verify our stories and they never follow up. The ‘fact checkers’ all refuse to get on a recorded phone or Zoom call since they don’t want to be exposed as being biased.
One strategy for changing this is that we’re going to run a series of ads. Each of the ads will feature a unique personality, like a Dr. Peter McCullough, a sports figure, doctors, victims and so on. They’ll relate their personal anecdotes for what’s happened to them. And they will say, ‘Look, before you get vaccinated, check the facts. Listen to the other side of the story.’
It’s a reasonable ask. And we’ll direct them where to go to hear the side of the story that the mainstream media aren’t allowing them to hear. And then we let them make up their own mind. People aren’t hearing the other side of the story, and the White House is helping suppress it. When the White House has a hit list of censorship, it’s very clear what is going on. When in history have we done that?
Do you ever see McCullough on CNN? No, because they want to give you only one side and they’re deliberately giving you only one side of it, and they know it. If they want to give the impression they are balanced, they’ll pick someone who isn’t an expert and interview them. Robert Malone is never going to be on CNN. Malone invented the mRNA vaccine and yet he doesn’t qualify to talk about it on CNN?
America used to be a country that embraced a diversity of views, and you had freedom of speech, you had freedom to express your opinion. You had the freedom to tell the truth. No more. That freedom has been taken away.
If you don’t agree with the mainstream narrative, you’re silenced. And so, what we’re going to do is run the series of ads, and we’ll only be able to run it on alternate media because the mainstream media won’t run our ads because the ads encourage people to hear the other side of the issue.”
More Information
Again, you can download Kirsch’s 177-page PDF, jam-packed with questions and data on the COVID “vaccine.” I also urge you to review his “False Narrative Takedown” (TFNT) series, which you can find on his Rumble channel.
You can also peruse his website, skirsch.io, or follow him on his social media accounts, which include Twitter, Gab, Telegram and LinkedIn. To keep on top of his latest investigations, you can subscribe to his Substack channel. If you can afford it, consider signing up for a paid subscription. Select articles can also be found on TrialSiteNews.
“Substack is really important because they don’t censor people who tell the truth,” Kirsch says. “So, I really encourage people to support platforms like Substack. I also get a portion of that, and any money I get, I will donate 100% to funding ads and to fighting this. If we can get 100,000 subscribers at $5 a month, that’s $500,000 a month we can spend to combat false narrative. That’s serious fire power.
People ask me, why am I doing this? I’m not making any money off of this. I have no conflicts of interest. I have no history as a conspiracy theorist or spreader of misinformation. We’ve lost all our friends.I was forced out of my job because I wanted to speak out against the vaccines.
I’m losing money on this because I’m funding a lot of the things out of my personal pocketbook. The donors that donated to the early treatment fund, none of them, not a single one, is supporting the effort to get the truth out about how dangerous these vaccines are and how wrong the mandates are.
My motivation is a 100% on saving lives. That’s my reward in life. If I can save one life, my life was worth living. If I can save 100 lives, even better. If I can save 100,000 lives, that is more meaningful than anything I’ve ever done or will do.”
August 4, 2021, CNN aired a hit piece on me based on a fabricated report by the Center for Countering Digital Hate (CCDH), which has since been refuted by Facebook
October 4, 2021, CNN aired a follow-up, urging Amazon to get into the book burning business by banning sale of my best-selling book, “The Truth About COVID-19: Exposing the Great Reset, Lockdowns, Vaccine Passports, and the New Normal”
They claim my book is full of “lies,” “misinformation” and “mistruths.” But not a single piece of evidence to back that up is presented
By and large, the COVID shot is unnecessary for most people, for the simple reason that most people aren’t at risk of dying from COVID-19
Your risk of dying from COVID-19 is less than 1%, and your absolute risk reduction from the COVID shot is right around 1% (maxing out at 1.3%). This means it is mathematically impossible for COVID “vaccines” to have a favorable impact on public health
August 4, 2021, CNN aired a hit piece on me based on a fabricated report by the Center for Countering Digital Hate (CCDH) — a report that has since been refuted by Facebook itself.1
According to the CCDH,2 I am No. 1 of a dozen individuals responsible for 65% of all anti-vaccine content on social media and should therefore be stripped of my First Amendment rights to free speech and banned from all platforms.
For their first broadcast, CNN reporter Randi Kaye, who wasn’t wearing a mask at the time, tracked me down as I bicycled around my home town to ask me about why I say masks don’t work, and whether I “feel responsible” for the deaths of unvaccinated people — a strange perspective indeed, considering the COVID shots CNN is pushing may have killed more than 200,000 otherwise healthy Americans so far.3
The U.S. Vaccine Adverse Event Reporting System (VAERS) had as of September 24, 2021, received 15,937 reports of deaths shortly after the COVID injection,4 and a report by Steve Kirsch provides compelling evidence that side effects are underreported by a factor of 41. That means the death toll may be closer to 250,000.
Does CNN regret having lured all of these people to their deaths by refusing to report anything negative about these experimental injections? At the end of that segment (below), Kaye decries the success of my best-selling book, “The Truth About COVID-19: Exposing the Great Reset, Lockdowns, Vaccine Passports, and the New Normal,” refusing to even state its title.
So far, the book has sold more than 250,000 copies, and all proceeds are being donated to the National Vaccine Information Center (NVIC), the oldest and largest vaccine safety advocacy group in the U.S.
CNN Takes Another Stab at My Book
October 4, 2021, CNN aired a follow-up on the book’s success — this time providing its title — while urging Amazon to get into the book burning business rather than being a book seller. Like something straight out of George Orwell’s “1984” newsspeak dictionary, CNN host Anderson Cooper said my book is loaded with “mistruths” about COVID. I guess “misinformation” doesn’t pack the same punch it once did.
They also still referred to me as a “superspreader of misinformation,” even though Facebook has published data showing that between the 12 of us “superspreaders,” we actually only account for a minuscule 0.05% of all vaccine-related content on that platform. As noted by Monika Bickert, vice president of Facebook content policy:5
“… these 12 people are responsible for about just 0.05% of all views of vaccine-related content on Facebook. This includes all vaccine-related posts they’ve shared, whether true or false, as well as URLs associated with these people.
The report6 upon which the faulty narrative is based analyzed only a narrow set of 483 pieces of content over six weeks from only 30 groups, some of which are as small as 2,500 users.
They are in no way representative of the hundreds of millions of posts that people have shared about COVID-19 vaccines in the past months on Facebook.
Further, there is no explanation for how the organization behind the report identified the content they describe as ‘anti-vax’ or how they chose the 30 groups they included in their analysis. There is no justification for their claim that their data constitute a ‘representative sample’ of the content shared across our apps.”
Show Us the Evidence, CNN
CNN uses the oldest propaganda trick in the book in its latest report. If you just spew out enough derogatory terms about your opponent, people will forget the fact that you provided zero proof to back up your position.
They claim my book is full of “lies,” “misinformation” and “mistruths.” But not a single piece of evidence to back that up is presented. They don’t even provide any specific examples of what these “lies” might be. My book is fully referenced, and none of those references has been publicly disputed or refuted as false.
A journalist accusing someone of lies had better well have proof of those lies. To produce a story without that proof is unconscionable and certainly not representative of honest journalism.
As Kaye mentions, CNN also contacted my publisher, Chelsea Green, for comment on a series of questions. Below are the answers provided by president and publisher Margo Baldwin to CNN’s AC360 producer Stephen Samaniego:
CNN Question: Why did Chelsea Green publish a book so full of misinformation?
Chelsea Green Answer: What misinformation? There is no misinformation as far as we are concerned. I might ask the same thing of CNN and the misinformation it perpetuates about the lab leak origins of the virus: www.cnn.com/2021/03/31/health/lab-leak-coronavirus-theory-comic-book-scn/index.html
CNN Question: Do you feel any responsibility at all for giving an author who is peddling lies about COVID a platform to profit from those lies?
Chelsea Green Answer: What lies? Please elaborate on the lies you are referring to.
CNN Question: Do you feel responsible for contributing to the misinformation that is out there about COVID and the vaccines?
Chelsea Green Answer: No, we feel we are contributing to the truth about COVID, as many other eminent scientists and doctors are also courageously doing.
CNN Question: How much money had the book grossed for Chelsea Green Publishing?
Chelsea Green Answer: I think you can figure that out for yourselves.
CNN Question: What was Dr. Mercola’s compensation for writing the book and how much has he earned from sales royalties?
Chelsea Green Answer: That is confidential information but Dr. Mercola has said publicly that he is donating all his earnings from the book to The National Vaccine Information Center, a nonprofit organization dedicated to vaccine safety.
In a statement accompanying her answers, Baldwin added:
“These are not serious journalistic questions. They are simply attempts by CNN to shut down debate and censor speech. We call it out for what it is: intimidation tactics to be used against anyone who dares to question the narrative that CNN is peddling.
Our responsibility is to the public and to stand up for free and open exchange of information. If you have questions about any of the facts in the book, check out the sources and examine the evidence instead of simply dismissing it as ‘misinformation.'”
Show Us the Lies
In an email response to Baldwin’s request for elaboration on the supposed lies he’s referring to, Samaniego stated:
“There are too many for me provide you a comprehensive list but a few top line ones that stick out …
That the vaccine trials were rigged, that the vaccines are part of unprecedented and dangerous experiment, that a large amount of data suggests that vaccines may be completely unnecessary, vaccines cannot prevent or reduce transmission or infection hospitalization or death. According to the CDC the vaccines are nearly 100% effective at preventing serious disease and death.”
Baldwin replied to this short-list with the following mainstream media links, none of which, by the way, has been accused of being superspreaders of mistruths:
“The trials were designed specifically to succeed. www.forbes.com/sites/williamhaseltine/2020/09/23/covid-19-vaccine-protocols-reveal-that-trials-are-designed-to-succeed/?sh=21270ac65247
Removing the placebo groups from vaccine trials will prevent accurate data from long term studies from being known. www.npr.org/sections/health-shots/2021/02/19/969143015/long-term-studies-of-covid-19-vaccines-hurt-by-placebo-recipients-getting-immuni
The experiments are continuing through 2027 as the FDA APPROVAL requires Pfizer to submit study results analyzing risk of myocarditis and pericarditis, and risk to long-term infant development in pregnant women. Study results reports will be submitted to the FDA for review on Oct 31, 2025 and May 31, 2027 respectively.
Nearly 60% of gravely ill patients are fully vaccinated, while stating the Pfizer vaccine is just 39% effective. www.sciencemag.org/news/2021/08/grim-warning-israel-vaccination-blunts-does-not-defeat-delta and www.cnbc.com/2021/07/23/delta-variant-pfizer-covid-vaccine-39percent-effective-in-israel-prevents-severe-illness.html.”
Are COVID Shots Necessary?
The one question Baldwin did not address was whether the COVID shots are even necessary. My next book, which will focus on the so-called COVID “vaccines,” will go into this question in great detail, but the fact of the matter is the shots are, by and large, unnecessary for most people, for the simple reason that most people aren’t at risk of dying from COVID-19.7,8,9,10,11
Data from a Wake Forest Baptist Health study12,13 suggest the overall death rate from COVID-19 is around 0.1%.14 Stanford University’s disease prevention chairman Dr. John Ioannidis has calculated the infection fatality rate as being between 0.05% and 1%, with a median of 0.25%. For those under the age of 45, the infection fatality rate is near zero, and between the ages of 45 to 70, it’s between 0.05% and 0.3%.15,16
Yet another study17 published in the Annals of Internal Medicine put the overall noninstitutionalized infection fatality rate at 0.26%. People younger than 40 have an infection fatality rate of 0.01%, while those 60 and older had a 1.71% risk of dying from the infection.
Now, if your risk of dying from COVID-19 is near zero, even if the injection is 100% effective at preventing death, you’re not getting any benefit since you weren’t at risk of dying in the first place.
This is not rocket science. So, CNN either cannot wrap their heads around these simple data points, or they ignore it because they don’t want you to understand just how small the risk of COVID-19 actually is, and how great the risks of the COVID injections are in comparison. If the latter is true, then they are complicit in the deaths of tens of thousands of Americans, and perhaps hundreds of thousands.
How Effective Are the COVID Shots, Really?
And, there’s more. A number of studies have also looked at the absolute risk reduction provided by the COVID shots, showing they’re near useless. While, at the outset, vaccine makers all boasted very high effectiveness for their COVID shots, independent reviews suggest their claims were massively overstated from the get-go.
As it turns out, they’re all using one of the simplest and oldest statistical tricks in the book: conflating relative and absolute risk reduction. Pfizer, for example, claimed its mRNA shot was 95% effective. How did they get that number? In trials reportedly involving tens of thousands of people, 170 were diagnosed with COVID-19 during the trial.
Of those, 162 were in the placebo group and eight were in the COVID shot group. From this, it is inferred that the shot prevented 154 out of 162 people from developing COVID-19. That’s 95%. However, this is the relative risk reduction. The absoluterisk reduction is actually less than 1%.18
When calculating absolute risk reduction, you compare the frequency of an outcome in the treatment group compared to untreated controls. As a hypothetical example, if 20% of the control group develops COVID-19, compared to just 12% of those who got the jab, then you have an absolute risk reduction of 8%.
That then means that if 100 people got the COVID shot, eight would not get COVID-19. This is the most accurate and helpful way to present data when you want people to be able to make an informed treatment choice; if you want to manipulate and deceive them, you would use the relative risk reduction.
Dr. Ron Brown published a paper detailing the problems with this kind of reporting bias specifically as it pertains to COVID-19 mRNA “vaccines.” In “Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials”19 Brown calculates the absolute risk reduction for Pfizer’s and Moderna’s injections, based on their own clinical trial data, so that we can compare them to the relative risk reduction reported by these companies. Here’s a summary:20
As noted by Brown, “Reporting absolute risk reduction measures is essential to prevent outcome reporting bias in evaluation of COVID-19 vaccine efficacy.”
In a July 1, 2021, commentary in The Lancet Microbe,21 Piero Olliaro, Els Torreele and Michel Vaillant also argue for the use of absolute risk reduction when discussing vaccine efficacy with the public. They too went through the calculations, coming up with the following:
The Data Prove COVID Shots Are Not a Viable Answer
As you can see, the absolute risk reduction for all of these COVID shots is below 1.3% (and those numbers can only go down as the effectiveness of the shots wane). And, as just mentioned, your risk of dying from COVID-19, provided you’re not ill and living in a nursing home, is around 0.25%.
So, again, if your risk of dying from COVID-19 is less than 1%, and your absolute risk reduction from the COVID shot is right around 1%, that tells us the mathematical possibility of these COVID “vaccines” having a favorable impact on public health is very close to zero.
Hence, stating that COVID shots may be unnecessary for most people is not a lie. It’s a commonsense conclusion that can be verified by anyone, in a number of different ways, using a number of different data sources. Unfortunately, CNN is no longer in the business of relaying verifiable data or facts.
Rather, they’re a propaganda mill for The Great Reset agenda, which needs vaccine passports to be implemented across the world. And in order for that to happen, people need to be convinced that COVID-19 is a lethal scourge that must be prevented, even if it costs us our freedom and the health, lives and livelihood of hundreds of millions of people.
I am donating all proceeds from this book to NVIC to help us protect our rights. NVIC works across all of the US, the are the oldest and most powerful voice we have in defending medical choice. Please help raise awareness by purchasing The Truth About COVID-19 while you can, and increase the visibility on Amazon so others will become aware of this important book before the censors have it banned. Thank you if you already have a copy, it has truly made a difference!
What Is the Current Rate for Reporting Vaxx Injuries?
By Dr. Joseph Mercola
In a Highwire exclusive, Deborah Conrad, a physician’s assistant (PA), blows the whistle on COVID jab injuries, and the fact that these injuries, by and large, are not being reported.
According to Conrad, shortly after the mass vaccination campaign began, she started seeing a surprising number of hospital patients who had recently received a COVID shot and were now testing positive for COVID-19.
In particular, patients were coming in with pneumonia, and this was happening even in the middle of the summer. It’s become so common, Conrad refers to 2021 as “the year of pneumonia.” Sepsis cases have also increased.
After the COVID jab rollout, she also noticed a marked increase in heart attacks, strokes, blood clots, gastrointestinal complaints and bleeds, appendicitis, pancreatitis and recurrent cancers. All of these were “noticeably increased,” she says, and “everybody seemed to notice it.”
Tomorrow, I will publish yet another bombshell video — a documentary called “Vaccine Secrets: COVID Crisis.” It’s the first episode of “The False Narrative Takedown Series,” produced by Steve Kirsch, executive director of the COVID-19 Early Treatment Fund. You won’t want to miss that one, as it complements and supports everything Conrad shared in this interview.
Most Health Care Workers Know Nothing about VAERS
Conrad, who has worked as a PA for 17 years, admits she knew nothing about the U.S. Vaccine Adverse Event Reporting System (VAERS) prior to the COVID vaccination campaign. This is the case with most health care providers. None of them were ever educated on how to identify potential vaccine injuries, how to report them, or that they have a legal requirement to report all emergency use vaccine injuries.
When it comes to conventional vaccines, reporting to VAERS is voluntary. Not so with emergency use vaccines, however. Vaccine injuries caused by a vaccine under Emergency Use Authorization (EUA) MUST be reported to VAERS by law. However, as noted by Conrad, there’s been absolutely no training on how to do so.
She was shocked to realize health care providers are actually required by law to report suspected EUA vaccine injuries, as none of the hospital staff had been instructed to do so. But on page 12 of Pfizer’s “Fact Sheet for Healthcare Providers Administering Vaccine,” it states that:
“The vaccination provider is responsible for mandatory reporting of the following to the Vaccine Adverse Event Reporting System (VAERS):
•vaccine administration errors whether or not associated with an adverse event,
•serious adverse events (irrespective of attribution to vaccination),
•cases of Multisystem Inflammatory Syndrome (MIS) in adults and children, and
•cases of COVID-19 that result in hospitalization or death.
Complete and submit reports to VAERS online at vaers.hhs.gov/reportevent.html. For further assistance with reporting to VAERS call 1-800-822-7967. The reports should include the words ‘Pfizer-BioNTech COVID-19 Vaccine EUA’ in the description section of the report.”
Doctors Have a Public Health Duty to Report Side Effects
In addition to a lack of education about VAERS, one of the reasons why so few physicians report suspected vaccine injuries is because there are no penalties for failing to fulfill your legal responsibilities. It’s essentially not enforced.
It’s worth noting that it is not the doctor’s job to decide whether an injury is caused by a vaccine or not. The language in VAERS is very clear on this. They are simply to report any adverse health condition that occurs after a vaccination has been given.
Over time, as reports accumulate, the FDA and CDC can then start to see potential associations, and if a particular condition occurs at high frequency after a particular vaccine is given, the link would then, theoretically at least, be investigated further. In short, VAERS function is to signal potential side effects that weren’t known before.
Naturally, collecting data on side effects is particularly crucial when dealing with a brand-new, never previously used medical product such as these mRNA and DNA-based COVID injections.
Every health care worker in the nation really ought to be on the lookout for potential side effects, and diligently fulfill their public health duty to report any and all health effects that occur within a month or two, at minimum, after the injections. We are, after all, in a mass experiment, and without rigorous data collection, how can we possibly understand what these injections are doing?
VAERS Is a Crucial Tool to Ensure Vaccine Safety
As soon as Conrad became aware of her responsibility to report side effects, she started filing reports. But there were so many that “quickly, that became a full-time job,” she says. Within a month, she’d already reported 50 suspected vaccine injuries.
Fact checkers typically dismiss VAERS data as “unreliable” because anyone can file a report. The fact that a patient experienced a problem after vaccination also does not mean that the vaccine was the cause. Such debunking attempts do not hold water, however.
First of all, filing a VAERS report is not a quick and easy task. It’s very time consuming and requires detailed data on blood work, symptoms, previous medical history, vaccine lot numbers and much more. What’s more, there’s no save feature, so you cannot walk away from it midstream, or the system will log you out and you have to start all over again.
So, to say VAERS is not optimized for ease of use and compliance is a profoundly serious understatement. Conrad, and many other doctors, have stated that the system will often also fail to authenticate once you hit “submit,” and erase the whole report. It’s almost like it’s was intentionally designed to discourage reporting.
There’s also no incentive to spend your days filing false reports, as there are penalties for doing so. This is in stark contrast to not filing a report, which carries no penalty. What’s more, while a patient or parent can file a report, most reports are done by medical professionals, and they’re not going to waste their time filing false reports.
Then there’s the actual purpose of VAERS, which as mentioned is to signal potential problems. It’s true any single report cannot be taken as proof that the vaccine caused a problem, but when you have thousands or tens of thousands of reports of a given effect, that’s a SIGNAL that there might be a link. This is clearly expressed on the FDA’s website:2
“The purpose of VAERS is to detect possible signals of adverse events associated with vaccines. VAERS collects and analyzes information from reports of adverse events (possible side effects) that occur after the administration of U.S. licensed vaccines.”
Avoiding Vaccine Hesitancy Deemed More Important Than Safety
Once Conrad started getting overwhelmed by the task of filing reports, she asked the hospital administration for help. She wanted the administration to educate the staff so that everyone could all pitch in and “do the right thing” by identifying injuries and filing reports.
Instead of getting the assistance she expected, she ran into a brick wall of resistance. The vaccination push was in full swing, and no one was willing to raise questions about vaccine safety, as it might promote vaccine hesitancy. Remarkably, promoting the idea that the shots are perfectly safe — even if untrue — was deemed more important than making sure patients were not being harmed by the millions.
Conrad then called her hospital’s president to ask why side effects were not routinely reported to VAERS as required by law. The president replied he believes “the position the system has taken is that each provider has the responsibility to report on their own patient.”
But how can they do that if they’re not educated about what they’re supposed to be reporting? Conrad asked. He told her “providers should educate themselves when they’re dealing with patients related to COVID vaccinations.”
After that, the risk management team told her she was no longer allowed to file reports on behalf of other doctors. She could only file reports for her own patients. She also received a written warning, saying she must support the hospital’s approach to the vaccine, per CDC and Department of Health guidance.
Historically, Vaccine Injuries Are Routinely Underreported
As explained by Conrad, as adult-care providers, they rarely deal with vaccinations, as adults receive very few vaccines. Pediatricians are typically the ones who administer vaccines, and they give them to babies and young children. Hence pediatricians may be more familiar with VAERS.
However, even among pediatricians, knowledge and use of VAERS is limited, and this has been known for over a decade. As noted in the so-called “Lazarus Report,” formally titled “Electronic Support for Public Health — Vaccine Adverse Event Reporting System,” published in late 2010:
“Preliminary data were collected from June 2006 through October 2009 on 715,000 patients, and 1.4 million doses (of 45 different vaccines) were given to 376,452 individuals.
Of these doses, 35,570 possible reactions (2.6 percent of vaccinations) were identified. This is an average of 890 possible events, an average of 1.3 events per clinician, per month.
These data were presented at the 2009 AMIA conference. In addition, ESP: VAERS investigators participated on a panel to explore the perspective of clinicians, electronic health record (EHR) vendors, the pharmaceutical industry, and the FDA towards systems that use proactive, automated adverse event reporting.
Adverse events from drugs and vaccines are common, but underreported. Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA).
Likewise, fewer than 1% of vaccine adverse events are reported. Low reporting rates preclude or slow the identification of ‘problem’ drugs and vaccines that endanger public health. New surveillance methods for drug and vaccine adverse effects are needed.
Barriers to reporting include a lack of clinician awareness, uncertainty about when and what to report, as well as the burdens of reporting: reporting is not part of clinicians’ usual workflow, takes time, and is duplicative.”
CDC’s New System Showed 1 in 10 Had Reactions
This report has an interesting backstory. In 2010, the CDC actually hired a company to automate VAERS. Any patient who received a vaccine within the Harvard Pilgrim HMO automatically had their medical records scanned for the next 30 days, such as diagnostic codes, lab tests and drug prescriptions.
Any health problem suggestive of an adverse event was then automatically uploaded into the VAERS database. Remarkably, preliminary data showed nearly 1 in 10 people suffered a reaction after vaccination, yet the official CDC mantra is that the risk for serious vaccine injury or death is 1 in 1 million.
Unfortunately, while the creation of VAERS in 1986 was an opportunity to get a firmer grasp of the number of potential vaccine reactions, injuries and deaths occurring after vaccinations given in the U.S., the CDC didn’t follow through, and the project fell by the wayside.
As noted by the authors, the plan to automate VAERS reporting didn’t happen because “the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.”
Why did the CDC drop this project? Don’t they want to protect public health from potentially dangerous products? Did they think the truth might destroy the vaccine industry?
Surprising Rise in Cancer and Other Odd Conditions
As mentioned, Conrad saw a dramatic rise in several different health problems as the COVID jabs were rolled out. One of the most surprising problems has been a sudden rise in cancers among vaccinated patients whose cancer had gone into remission before the jab.
Bigtree points out he’s spoken with a number of oncologists who have made the same observation in their practices. These cancers tend to be very sudden in onset and highly aggressive, often leading to death.
She’s also seeing new cancers that appear “out of nowhere,” and rarer types of cancer, such as solid organ tumors that kill the patient before a biopsy can even be taken.
Blood clots and strokes have also skyrocketed, and these occur even in patients who are on maximum doses of anticoagulants. Odd and unusual neurological problems with seizures and tremors are also becoming more commonplace, as is pneumonia and sepsis.
Are We in a Pandemic of the Unvaccinated?
When asked if a majority of the patients in her hospital are unvaccinated — which is what we’re being told — she says no, quite the opposite. She’s been tracking the numbers for a couple of months, and as just one example, on one particular day in July, of the 35 patients admitted, 30 were fully vaccinated, and all of the seven patients in the intensive care unit were fully vaccinated.
This despite the fact that, at that time, the county vaccination rate was only between 40% and 45%. She points out that these vaccinated patients were not all COVID-19 patients, but were admitted for all sorts of health issues. Many vaccinated patients have also been readmitted several times since they got their shot.
While Conrad has done everything she can to protect public health up until now — having filed more than 120 VAERS reports so far — she won’t be fighting on the frontlines any longer. She’s being let go from her job at the end of September 2021 for refusing to get the COVID shot. After everything she’s seen, “I’m more afraid of the vaccine than I am of COVID,” she says.
The Likely Result of This Tyrannical Intervention
This is the ultimate irony. Conrad is clearly one of the most compassionate, high integrity and absolutely committed health professionals in that hospital and they are firing her for adhering to her constitutional rights. I believe this is precisely the behavior that will ultimately lead to the self-destruction of our society.
You simply can’t fire tens of millions of some of the brightest and most honest people in the country who adhere to personal freedom and liberty and not expect it to have devastating consequences. Who will be left to do the work? The majority of these people being terminated are highly trained professionals that can’t be easily replaced.
It is clear they don’t understand the results of these tyrannical interventions. It is beyond evident that we are in for some very rocky times with massive shortages as people are fired from their jobs. So, be prepared folks, and stock up as if you were expecting a hurricane and knew you’d have no access to outside help for three to six months. I hope this doesn’t happen, but everything is pointing to this outcome.
Vaccine-Injured Patients Want To Be Heard
The sad truth is, we’re in an epidemic of vaccine injuries, and injured patients are now routinely ignored by the very people who encouraged them to get the shot. To get an idea of what the risks actually are, check out some of the cases reported to nomoresilence.world4 and c19vaxreactions.com,5 two websites dedicated to giving a voice to those injured by COVID shots.
You can also browse through more than 246,000 comments left on a Facebook post by WXYZ-TV Channel 7.6,7 They asked people who had lost an unvaccinated loved one to COVID-19 to contact them for a story, but what they got was an avalanche of stories of vaccine injuries and deaths instead. Below is a sampling of comments posted on the site:
“How about doing a story about my uncle who was in fine shape until he got vaccinated. Or my boss’s uncle who was healthy and in his 50s, then died suddenly a week after getting vaccinated.”
“My sister-in-law’s father died of a stroke 48H after Moderna vax. He was active and healthy.”
“The shot murdered my friend three weeks after he got it.”
“I know 2 women who had strokes aright after their shot.”
“We lost an uncle to heart inflammation 2 days after he received the vaccine.”
“Lost a very dear man after his second dose of the vaccine and he said he regretted getting it and he advised me not to get it. How about reporting on those? He died of a brain aneurysm, and was a very healthy man.”
“My beautiful mother passed away recently, 23 days after having the first AstraZeneca shot (that I didn’t know she was getting). ‘Immunization’ was the ‘cause of death’ on her death certificate.”
“I now know more people injured by the vaccine than people who even had covid.”
“No, but I know of two people who died from Covid after being fully vaccinated.”
“My uncle passed away 3 months after his second shot. He was diagnosed with stage 4 colon cancer, had surgery, was released to rehab and then died of a blood clot. Thanks Pfizer.”
“I know of two women who had miscarriages within 2 days of taking it.”
As noted by one commenter, “Doesn’t sound like you’re getting the story you need judging by the vast majority of these comments about vaccine losses and side effects. Since there is such an overwhelming outpouring of vaccine reactions, maybe do a story on that?”
Spike Protein Is Very Dangerous, It’s Cytotoxic (Robert Malone, Steve Kirsch, Bret Weinstein)
By AveFe | Vimeo
Dr. Robert Malone is the inventor of mRNA Vaccine technology.
Mr. Steve Kirsch is a serial entrepreneur who has been researching adverse reactions to COVID vaccines.
Bret talks to Robert and Steve about the pandemic, treatment and the COVID vaccines.
Here’s what others had to say:
Emmanuel Marshall
It is a sign of troubling times when you look at a video and say “Huh, I’m surprised this isn’t banned yet”..
Paddy
When governments need to bully you into making a medical decision that should be yours alone to make then you know you are dealing with a shitty product. No medical PHD’s are necessary to spot the fraud.
yankee way farms
I already had covid. I followed restrictions for a year wore my mask and caught covid right before the vaccine was available. I had a very mild case and only lost my sense of taste and smell I quarantined and then I was told to wait to get the vaccine. Now all the data is showing natural immunity is equal to or better then vaccine immunity. So why should anyone with natural immunity be forced to vaccinate? Why are they ignoring natural immunity? Nevermind them telling the fully vaccinated to continue to mask. This makes no sense and our government is going full dictator.
Ryan Caputo
My Dad, who is a doctor, spent 3 days in the ICU with a very high pulse rate (enough to shut down organs) after getting vaccinated at a doctors convention, thank god he survived.
Seamus McDonnell
The fact that it is still being forced onto us is truly insane when you consider explanations like this.
Hearts Fanatic101
Truth does not mind being questioned, whereas a lie does not like being challenged.
ali bakr
Covid hysteria seems to have removed all memory of what getting sick was like before covid.
Who is Maddie De Garay and Why is Just One Sadly of Many?
By Staff Reporter
Maddie De Garay was 1 out of 1131 in the treatment arm of the Pfizer trial on children. She was 12 at the time. Within 24 hrs of her second Pfizer shot she was paralyzed. Pfizer reported her case as “abdominal pain” instead of “permanent paralysis”. She was never ejected from the trial.
FDA commissioner Janet Woodcock promised an investigation. To date Maddie hasn’t been contacted by the FDA or the CDC in regards to the fraud. She has received no compensation.
Steve Kirsch recently raised this in the FDA held Vaccine Advisory Committee meeting on September 17, 2021 to discuss authorizing a third Pfizer COVID-19 “booster shot.”
Alarming FDA Public Hearing. Listen to the Chilling Words of Dr Fraiman. Then the Very Important Slides From Steve Kirsch, the Executive Director of BS 19 Early Treatment
By Reignite Democracy Australia
Alarming FDA public hearing
Listen to the chilling words of Dr Fraiman. Then the very important slides from Steve Kirsch, the Executive Director of Covid 19 Early Treatment.
FDA Experts Reveal the BS-19 Vazzines Are Killing at Least 2 People for Every 1 Life They Save As They Vote 16 – 2 Against the Approval of Booster Shots.
By Daily Expose
FDA experts have unexpectedly voted against approving Covid-19 vaccination boosters for anyone over the age of 16 in the USA, citing a lack of long term data and stating that the risks do not outweigh any benefits because the Covid-19 vaccines are killing at least 2 people for every 1 life saved.
In a live broadcast conducted on the 17th September the Food and Drug Administration vaccine advisory committee met to debate and vote on Pfizer and BioNTech’s application to offer booster shots to the general public. The meeting lasted over 8 hours and contained some shocking revelations.
Dr Joseph Fraiman, an emergency medicine physician in New Orleans, spoke for several minutes during the meeting and revealed that no clinical evidence exists to disprove claims that the Covid-109 vaccines are harming more people than they save.
“We need your help on the front lines, to stop vaccine hesitancy. Demand the booster trials are large enough to find a reduction in hospitalisations.
“Without this data we the medical establishment cannot confidently call out anti-Covid-vaccine activists who publicly claim the vaccines harm more than they save especially in the young and healthy.
“The fact we do not have the clinical evidence to say these activists are wrong should terrify us all”.
Dr Joseph Fraiman was then followed by Steve Kirsch, Executive Director of the Covid-19 Early Treatment Fund, who revealed that the Covid-19 vaccines more people than they are saving.
“I’m going to focus my remarks today on the elephant in the room that nobody likes to talk about, that the vaccines kill more than they save.
“We were led to believe that the vaccines were perfectly safe but this is simply not true, for example there are four times as many heart attacks in the treatment group in the Pfizer 6 month file report, that wasn’t just bad luck.VAERS shows heart attacks happen 71 times more often following these vaccines compared to any other vaccine,”
Steve Kirsch then continued his presentation by showing a slide titled ‘Excess Death: Life ratio is UNACCEPTABLE’. The slide shows how many excess deaths were required following vaccination to save one life due to Covid-19.
“Only the VAERS (Vaccine Adverse Event Reporting System) are statistically significant, but the other numbers are troubling.” said Steve Kirsch.
“Even if the vaccines have 100% protection, it still means we kill 2 people to save 1 life.
“Four experts did analysis using completely different non US data sources and all of them came up with approximately the same number of excess vaccine related deaths, about 411 deaths per million doses. That translates into 115,000 people have died (due to the Covid-19 vaccines).”
The Executive Director of the Covid-19 Early Treatment Fund then pointed out some serious concerns over data coming out of Israel.
“The real numbers confirm that we kill more than we save. And I would love to look at the Israel ministry of health data on the 90+ year olds where we went from a 94.4% vaccinated group to 82.9% vaccinated in the last 4 months. I
“in the most optimistic it means that 50% of the vaccinated people died and 0% of unvaccinated people died. Unless you can explain that to the public you cannot approve the boosters.”
Peter Marks, FDA’s top vaccine regulator, then asked committee members to examine “the totality of the evidence in order to make your recommendation for us,”.
Following the evidence they responded with a resounding no voting 16 – 2 against advising the agency to roll-out booster shots to anyone over the age of 16.