Former Pro Calls for “Investigation” After Another Football Player Suddenly Collapses
By Paul Joseph Watson
A former professional Premier League footballer has called for an investigation after yet another player suddenly collapsed in the middle of a match last night.
Sheffield United midfielder John Fleck fell to the ground during his team’s game at Reading and had to be taken off on a stretcher after receiving lengthy treatment and being given an oxygen mask.
The 30-year-old Scottish international “went down unchallenged before team-mates quickly waved medics on,” reports BBC News.
Fleck was taken to hospital where he is said to be in good condition.
The player becomes yet another unfortunate addition to a lengthy list of footballers and other top athletes who have suddenly collapsed on the field of play in recent months.
As we previously highlighted, major German newspaper Berliner Zeitung recently published a report seeking to answer why an “unusually large number of professional and amateur soccer players have collapsed recently.”
The article listed a large number of recent cases of footballers who have had heart problems or collapsed on the field, in some cases leading to death.
That list includes Barcelona’s Sergio Aguero, who suffered breathing difficulties during Barca’s LaLiga clash with Alaves last month. Although the club have denied rumors Aguero is set to retire, he will definitely be out of action for months.
Other professional athletes have also recently suffered similar health problems, including 24-year-old Slovak hockey player Boris Sádecký, who tragically died after collapsing on the ice during a match last month.
Former England and Southampton player Matt Le Tissier responded to the news of Fleck’s collapse by calling for a proper investigation.
“How many more more sports people need to collapse on the pitch before an investigation takes place,” tweeted the ex-Premier League star.
It is not known whether John Fleck had taken the COVID-19 vaccine.
Meanwhile, according to a report by Dr. Yaffa Shir-Raz, there has been a “5-fold increase in sudden cardiac deaths of FIFA players in 2021.”
“So what is causing this sudden epidemic?” asks Shir-Raz.
Jordan Hayes: 33-year-old New York Man Dead 14 Weeks After C0VID-19 Vaxxine
By The COVID Blog
Mr. Jordan Hayes
NEW YORK — A 33-year-old New York husband and apparent dog lover is dead in another case of death after virtue signaling.
Mr. Jordan Hayes received his first dose of experimental mRNA on or around February 23, according to his Facebook page. It’s unclear which shot he received. But Pfizer and Moderna were the only two experimental injections available for emergency use in the United States at the time.
The since-deleted Facebook post appears to show a photo of a vaccine clinic. Mr. Hayes not only said that the non-vaccinated are failing society, but also called them “idiots” and “morons.” He emphasized that his message was being spoken “with all of my heart.” Passed away 14 Weeks After COVID-19 “Vaccine”
Michael Mitchell: 65-year-old Receives Both Sinovac Injections, Then Third Pfizer “Booster” Shot, Dead Six Days Later
By The COVID Blog
Mr. Mike Mitchell
FETHIYE, TURKEY — A 65-year-old actor, bodybuilder and former Mr. Universe is dead after proudly admitting his voluntary guinea pig status.
Mr. Michael Mitchell received his first experimental Sinovac Coronavac “inactivated virus” injection on February 22, according to his Facebook page. Coronavac is used pretty much everywhere (including Mexico and the Philippines) except the United States, Russia and Western Europe. He received the second injection on March 20. He reported no apparent adverse effects. But Mr. Mitchell and a friend immediately wondered if the China-made Coronavac injections would suffice for international travel.
The final sentence in the July 21 post reads, “P.S. I have had three vaccinations of different brands, so we may learn more about a way forward.”
Mr. Mitchell died the next day, Friday, July 22 in a marina cabin near his house boat. The marina manager checked on the actor after he was inside the cabin for an unusually long time. Mr. Mitchell was found unresponsive, lying on the floor.
Brent Henley: 63-year-old Louisiana Man Quiet for Months After Vaxxination of Johnson & Johnson
By The COVID Blog
Mr. Brent Henley
LAFAYETTE, LOUISIANA — A 63-year-old CEO is dead in a near-term case that is both strange and sad.
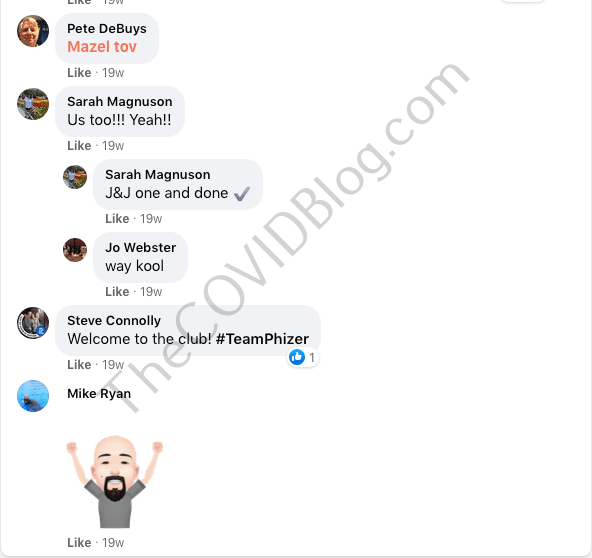
Mr. Brent Henley declared via Facebook, “vaccination complete” on March 24. He did not specify which experimental injection he received. But Mr. Henley made no reference to prior or subsequent injections, thus it was likely the then-recently authorized Johnson & Johnson injection. The comments read like a group of sports fans declaring their loyalty and cheering on their hometown teams.
Mr. Henley posted absolutely nothing about COVID-19, masks, experimental injections, etc. for almost exactly four months thereafter. He posted a lot about his job as CEO of the Pyramid Group and SIMSOC. The latter is apparently a big part of what his company does. Mr. Henley also posted a lot about his grandchildren and sports. That all changed in late July.
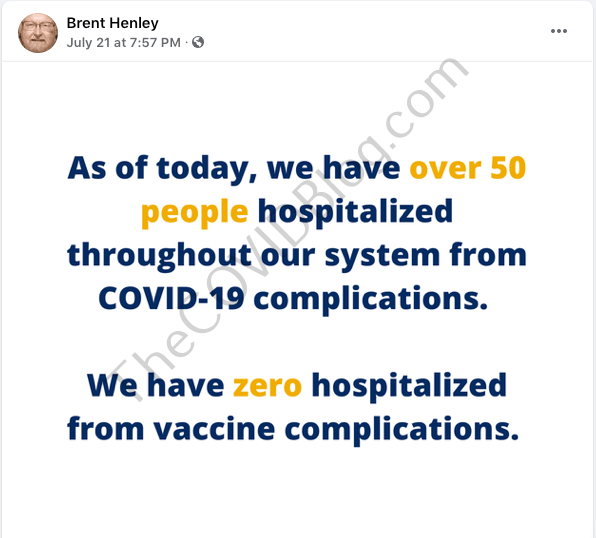
He posted blatant mainstream media propaganda on July 21. The post insinuated that COVID-19 is bad and deadly, while there is absolutely no risk in getting injected with the experimental shots.
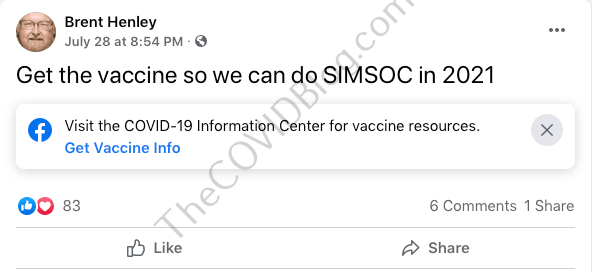
One week later, he wrote that everyone should “get the vaccine so we can do SIMSOC in 2021.”
Three days later, he posted something that is difficult to decipher. But it is essentially some sort of false-equivalency telling everyone to wear masks.
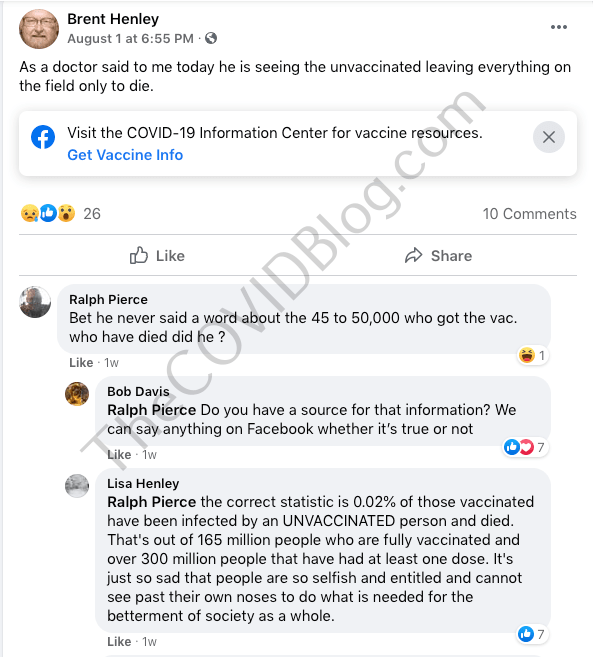
The most disturbing, and direct shot at the non-vaccinated, came on August 1. Mr. Henley insinuated that “the unvaccinated” are in danger of dying. One of Mr. Henley’s friends attempted to tell the truth about the experimental injections in the comments, only to be belittled and dismissed.
His final Facebook post was about SIMSOC on August 5. He died on August 8.
Death anticipation and/or vaccine rage?
Mr. Henley died “after a sudden and brief illness,” a description we’ve written many times on this blog. All near-term deaths we’ve covered thus far occurred between 10 and 14 weeks after the injection(s). This one was about 18 weeks after the injection. These deaths, as posited by Dr. Sherri Tenpenny, are likely caused by antibody-dependent enhancement (ADE). But there’s another glaring phenomenon in the case of Mr. Henley.
It seemed out of character and strange for him to start belittling and insulting the non-vaccinated towards the end of his life. There are no virtue-signaling posts, except the “I’m vaxxed” one, on either his Facebook or Twitter from July 2020 until the first one in late July 2021.
Perhaps Mr. Henley could feel something wrong with his body, knew he was dying and went out “screaming and kicking” if you will. This blogger has also posited the mind-control aspect via the Bill Gates-Microsoft body activity data apparatus. Again the virtue signaling just seemed totally out of character for this person based on his social media history.
Mr. Henley is survived by his wife, adult children and grandchildren.
One of the most commonly used tricks to make a drug look more effective than it is in a real-world setting is to conflate absolute and relative risk reduction. While AstraZeneca boasted a relative reduction of 100%, the absolute reduction was 0.01%. For the Pfizer shot, the relative risk reduction was initially 95%, but the absolute risk reduction was only 0.84%
In AstraZeneca’s trial, only 0.04% of people in the vaccine group, and 0.88% in the placebo group were infected with SARS-CoV-2. When the background risk of infection is that low, even a 100% absolute risk reduction becomes near-meaningless
Research shows the majority of SARS-CoV-2-specific antibodies in obese COVID-19 patients are autoimmune and not neutralizing. This means that if you’re obese, you’re at risk of developing autoimmune problems if you get the natural infection. You’re also at higher risk of a serious infection, as the antibodies your body produces are not the neutralizing kind that kill the virus. Does the same hold true for antibodies made in response to the COVID jab?
At nearly 72%, Vermont has the highest rate of “fully vaccinated” residents in the country, yet COVID cases are suddenly surging to new heights. During the first week of November 2021, cases increased by 42%. The hospital admission rate for fully vaccinated patients increased by 8%, while the admission rate for those who were not fully vaccinated decreased by 15%. Local health authorities blame the surge on the highly infectious delta variant, which would be odd if true, since the first delta case in Vermont was detected back in mid-May
Data from physician assistant Deborah Conrad show vaccinated people — counting anyone who got one or more shots, regardless of time since the injection — are nine times more likely to be hospitalized than the unvaccinated
In a November 12, 2021, blog post,1 Maryanne Demasi, Ph.D., reviews how the benefits of the COVID-19 shots have been exaggerated by the drug companies and misrepresented to the public by an uncritical media. She has previously given many lectures on how the drug companies conflated absolute and relative risks for statin drugs.2
Demasi was a respected Australian science presenter at ABC television until she produced a Catalyst report on the dangers of Wi-Fi and cellphones. In the wake of the controversy it raised, she and 11 of her staff members were axed and the episode retracted.3 That was 2016. Today, Demasi is one of the few professional journalists seeking and publishing the truth about COVID-19.
Absolute Versus Relative Risk Reduction
In her post, Demasi highlights one of the most commonly used tricks in the book — conflating absolute and relative risk reduction. As noted by Demasi, AstraZeneca and Australia’s health minister, Greg Hunt, claimed the AstraZeneca injection offered “100% protection” against COVID-19 death. How did they get this number? Demasi explains:4
“In the trial5 of 23,848 subjects … there was one death in the placebo group and no deaths in the vaccinated group. One less death out of a total of one, indeed was a relative reduction of 100%, but the absolute reduction was 0.01%.”
Similarly, Pfizer’s COVID shot was said to be 95% effective against the infection, but this too is the relative risk reduction, not the absolute reduction. The absolute risk reduction for Pfizer’s shot was a meager 0.84%.
It’s worth noting that an incredibly low number of people were infected in the first place. Only 8 out of 18,198 vaccine recipients developed COVID symptoms (0.04%), and 162 of the 18,325 in the placebo group (0.88%).
Since your risk of COVID was minuscule to begin with, even if the shot was able to reduce your absolute risk by 100%, it would still be trivial in real-world terms.
According to Gerd Gigerenzer, director of the Harding Centre for Risk Literacy at the Max Planck Institute, only quoting the relative risk reduction is a “sin” against transparent communication, as it can be used as a “deliberate tactic to manipulate or persuade people.” Demasi also quotes John Ioannidis, professor at Stanford University, who told her:6
“This is not happening just for vaccines. Over many decades, RRR [relative risk reduction] has been the dominant way of communicating results of clinical trials. Almost always, RRR looks nicer than absolute risk reductions.”
Demasi continues:7
“When asked if there was any justification for misleading the public about the vaccine’s benefits to encourage uptake, Prof Ioannidis rejected the notion.
‘I don’t see how one can increase uptake by using misleading information. I am all in favor of increasing uptake, but this needs to use complete information, otherwise sooner or later incomplete information will lead to misunderstandings and will backfire,’ says Ioannidis.
The way authorities have communicated risk to the public, is likely to have misled and distorted the public’s perception of the vaccine’s benefit and underplayed the harms. This, in essence, is a violation of the ethical and legal obligations of informed consent.”
US Health Authorities Have Misrepresented the Data
U.S. health authorities, like Australia’s, are guilty of misrepresenting the data to the public. In February 2021, Centers for Disease Control and Prevention director Rochelle Walensky co-wrote a JAMA paper8 which stated that “Clinical trials have shown that the vaccines authorized for use in the U.S. are highly effective against COVID-19 infection, severe illness and death.”
Alas, “there were too few deaths recorded in the controlled trials at the time to arrive at such a conclusion,” Demasi writes.9 This observation was made by professor Peter Doshi, associate editor of The BMJ, during Sen. Ron Johnson’s Expert Panel on Federal Vaccine Mandates, November 1, 2021.10 During that roundtable discussion, Doshi stated that:
“The trials did not show a reduction in deaths, even for COVID deaths … Those who claimed the trials showed that the vaccines were highly effective in saving lives were wrong. The trials did not demonstrate this.”
Indeed, the six-month follow-up of Pfizer’s trial showed 15 deaths in the vaccine group and 14 deaths in the placebo group. Then, during the open label phase, after Pfizer decided to eliminate the placebo group by offering the actual shot to everyone who wanted it, another five deaths occurred in the vaccine group.
Two of those five had originally been in the placebo group, and had taken the shot in the open label phase. So, in the end, what we have are 20 deaths in the vaccine group, compared to 14 in the placebo group. We also have the suspicious fact that two of the placebo participants suddenly died after getting the real deal.
How You Express Effect Size Matters
As noted in a July 2021 Lancet paper,11 “fully understanding the efficacy and effectiveness of vaccines is less straightforward than it might seem. Depending on how the effect size is expressed, a quite different picture might emerge.”
The authors point out that the relative risk reduction really needs to “be seen against the background risk of being infected and becoming ill with COVID-19, which varies between populations and over time.” This is why the absolute risk reduction figure is so important:12
“Although the RRR considers only participants who could benefit from the vaccine, the absolute risk reduction (ARR), which is the difference between attack rates with and without a vaccine, considers the whole population …
ARR is also used to derive an estimate of vaccine effectiveness, which is the number needed to vaccinate (NNV) to prevent one more case of COVID-19 as 1/ARR. NNVs bring a different perspective: 81 for the Moderna–NIH, 78 for the AstraZeneca–Oxford … 84 for the J&J, and 119 for the Pfizer–BioNTech vaccines.
The explanation lies in the combination of vaccine efficacy and different background risks of COVID-19 across studies: 0.9% for the Pfizer–BioNTech … 1.4% for the Moderna–NIH, 1.8% for the J&J, and 1.9% for the AstraZeneca–Oxford vaccines.
ARR (and NNV) are sensitive to background risk — the higher the risk, the higher the effectiveness — as exemplified by the analyses of the J&J’s vaccine on centrally confirmed cases compared with all cases: both the numerator and denominator change, RRR does not change (66–67%), but the one-third increase in attack rates in the unvaccinated group (from 1.8% to 2.4%) translates in a one-fourth decrease in NNV (from 84 to 64) …
With the use of only RRRs, and omitting ARRs, reporting bias is introduced, which affects the interpretation of vaccine efficacy.
When communicating about vaccine efficacy, especially for public health decisions such as choosing the type of vaccines to purchase and deploy, having a full picture of what the data actually show is important, and ensuring comparisons are based on the combined evidence that puts vaccine trial results in context and not just looking at one summary measure, is also important.”
The authors go on to stress that comparing the effectiveness of the COVID shots is further hampered by the fact that they use a variety of different study protocols, including different placebos. They even differ in their primary endpoint, i.e., what they consider a COVID case, and how and when diagnosis is made, and more.
“We are left with the unanswered question as to whether a vaccine with a given efficacy in the study population will have the same efficacy in another population with different levels of background risk of COVID-19,” the authors note.
One of the best real-world examples of this is Israel, where the relative risk reduction was 94% at the outset and an absolute risk reduction of 0.46%, which translates into an NNV of 217. In the Phase 3 Pfizer trial, the absolute risk reduction was 0.84% and the NNV 119.13 As noted by the authors:14
“This means in a real-life setting, 1.8 times more subjects might need to be vaccinated to prevent one more case of COVID-19 than predicted in the corresponding clinical trial.”
SARS-CoV-2 Specific Antibodies Pose Danger for the Obese
In related news, a recent study15 published in the International Journal of Obesity warns that “the majority of SARS-CoV-2-specific antibodies in COVID-19 patients with obesity are autoimmune and not neutralizing.”
In plain English, if you’re obese, you’re at risk of developing autoimmune problems if you get the natural infection. You’re also at higher risk of a serious infection, as the antibodies your body produces are not the neutralizing kind that kill the virus. As explained by the authors:16
“SARS-CoV-2 infection induces neutralizing antibodies in all lean but only in few obese COVID-19 patients. SARS-CoV-2 infection also induces anti-MDA [malondialdehyde, a marker of oxidative stress and lipid peroxidation] and anti-AD [adipocyte-derived protein antigens] autoimmune antibodies more in lean than in obese patients as compared to uninfected controls.
Serum levels of these autoimmune antibodies, however, are always higher in obese versus lean COVID-19 patients. Moreover … we also evaluated the association of anti-MDA and anti-AD antibodies with serum CRP and found a positive association between CRP and autoimmune antibodies.
Our results highlight the importance of evaluating the quality of the antibody response in COVID-19 patients with obesity, particularly the presence of autoimmune antibodies, and identify biomarkers of self-tolerance breakdown. This is crucial to protect this vulnerable population at higher risk of responding poorly to infection with SARS-CoV-2 than lean controls.”
Now, these findings apply to obese people who develop the natural infection, but it makes one wonder whether the same holds true for the COVID jab. If the antibodies produced in response to the actual virus are primarily autoantibodies, will obese people develop autoantibodies instead of neutralizing antibodies in response to the COVID shot as well?
For clarity, an autoantibody is an antibody that is directed against one or more of your own body’s proteins. Many autoimmune diseases are caused by autoantibodies that target and attack your own tissues or organs.
So, this is no small concern, seeing how the mRNA in the COVID shots (and subsequent SARS-CoV-2 spike protein, which is what your body produces antibodies against) gets distributed throughout your body and accumulates in various organs.17,18
At this point, there’s an overwhelming amount of evidence showing the COVID shots are not working. What little protection you do get clearly wanes within a handful of months, and may leave you worse off than you were before. We’re seeing data to this effect from a number of different places.
In the U.S., we can now look at Vermont.19 At nearly 72% vaccinated, it has the highest rate of “fully vaccinated” residents in the country, according to ABC News,20 yet COVID cases are now suddenly surging to new heights.
U.S. Centers for Disease Control and Prevention data show Vermont had the 12th highest COVID case rate in the nation as of November 9, 2021. Over the previous seven days, cases had increased by 42%. It couldn’t have been due to a surge in testing, though, as the weekly average of tests administered had only increased by 9% in that time.
What’s more, during that first week of November, the hospital admission rate for patients who were fully vaccinated increased by 8%, while the admission rate for those who were not fully vaccinated actually decreased by 15%.
Keep in mind that you’re not considered “fully vaccinated” until two weeks after your second injection. If you got your second dose a week ago and end up in the hospital with COVID symptoms, you’re counted as unvaccinated. This gross manipulation of reality makes it very difficult to interpret the data, but even with this manipulation it is beyond obvious that the vaccines are failing.
Overall, the case rate in Vermont is FAR higher now than it as in the fall of 2020, when no one had gotten the “vaccine.” According to Vermont health commissioner Dr. Mark Levine, the surge is occurring primarily among unvaccinated people in their 20s and children aged 5 through 11 — a curious coincidence, seeing how the shots are just now being rolled out for 5- to 11-year-olds.
Levine blames the surge on the highly infectious delta variant, but delta has been around for months already. The first case of delta in Vermont was identified in mid-May 2021.21 Surely, it wouldn’t have taken six months for this most-infectious of variants to make the rounds and cause an unprecedented spike?
Two clues are given by Levine, however, when he admits that a) Vermont has one of the lowest rates of natural immunity in the U.S. and b) protection is waning among those who got the COVID shot early to mid-year. Breakthrough cases among the fully vaccinated shot up 31% during the first week of November.22
Fully Vaxxed Are Nine Times More Likely To Be Hospitalized
Coincidentally, data from physician assistant Deborah Conrad, presented by attorney Aaron Siri23 October 17, 2021, shows vaccinated people are nine times more likely to be hospitalized than the unvaccinated.
The key, however, was in what they counted as vaccinated. Rather than only including those who had gotten the shot two weeks or more before being hospitalized, they simply counted those who had one or more shots, regardless of when, as vaccinated. This gives us an honest accounting, finally! As explained by Siri:24
“A concerned Physician Assistant, Deborah Conrad, convinced her hospital to carefully track the COVID-19 vaccination status of every patient admitted to her hospital. The result is shocking.
As Ms. Conrad has detailed, her hospital serves a community in which less than 50% of the individuals were vaccinated for COVID-19 but yet, during the same time period, approximately 90% of the individuals admitted to her hospital were documented to have received this vaccine.
These patients were admitted for a variety of reasons, including but not limited to COVID-19 infections. Even more troubling is that there were many individuals who were young, many who presented with unusual or unexpected health events, and many who were admitted months after vaccination.”
Despite these troubling findings, health authorities ignored Conrad when she reached out. In mid-July 2021, Siri’s law firm also sent formal letters to the CDC, the Health and Human Services Department and the U.S. Food and Drug Administration on Conrad’s behalf,25 and those were ignored as well.
“This again highlights the importance of never permitting government coercion and mandates when it comes to medical procedures,” Siri writes.26
Now, one of the most shocking details gleaned from Conrad’s data collection, which Siri failed to make clear but Steve Kirsch highlights in a recent substack post is that:27
“The only way you can get those numbers is if vaccinated people are 9 times more likely to be hospitalized than unvaccinated. It is mathematically impossible to get to those numbers any other way. Period. Full stop. This is known as an ‘inconvenient truth.’”
Indeed, the more data we gain access to, the worse it looks for these COVID shots. Unfortunately, those who push them seem hell-bent on ignoring any and all data that don’t support their stance.
Worse, it seems data and statistics are being intentionally manipulated by our health authorities to present a false picture of safety and effectiveness. All such tactics are indefensible at this point, and people who believe the official narrative without doing their own research do so at their own risk.
Joey Mishkin: 35-year-old Florida Single Father Receives Pfizer mRNA Injection to Save His Job, Suffers Massive Heart Attack, Dead 12 Days Later
By The COVID Blog
Mr. Joseph Mishkin
MIAMI — A 35-year-old single father is dead because society and his employer coerced him into self-poisoning in order to feed his family.
Mr. Joseph “Joey” Mishkin received his first Pfizer mRNA injection on October 1, according to his aunt, Renée Grossman. He got the shot because of an ultimatum from his employer. The next day, Mr. Mishkin suffered sudden cardiac arrest (heart stopped beating) while hanging around the pool at his newly-purchased home. Paramedics were able to get his heart pumping again upon arrival at the scene. But his heart stopped again in transit to the hospital.
Doctors placed Mr. Mishkin on a ventilator that night. It kept him “technically” alive for several more days. But the damage was done from all the heart stoppages and lack of oxygen to his brain and other organs. Mr. Mishkin passed away on October 12.
Danny Madry: Fully-Vaxxinated Florida Man With Leukemia Dies of C0VID-19
By Briona Arradondo
Mr. Danny Madry
APOLLO BEACH, Fla. – An Apollo Beach father living with leukemia died from C0V-19 last week despite being fully vaccinated, and his son said he hopes his dad’s situation motivates others with health conditions to rethink their risk.
Daniel Madry, 61, enjoyed spending time on a boat around Tampa Bay and hanging out with family playing music.
“He played the guitar a little bit. He would always send me random videos and it was always fun watching him get better and better,” said Mike Madry of Tampa, one of Madry’s sons.
Mike said his dad got more health conscious after he was diagnosed with chronic lymphocytic leukemia in May 2020.
“That really changed his thinking on diet, so he started cutting out all sugar and immediately started working out again as well and the transformation from 2018 to now was incredible,” said Mike. “He really had a six-pack, and he was 61 years old. He was in incredible shape.”
Mike Madry said his father was strict with masking and social distancing as well during the pandemic. So when the chance came for his father to ease up on safety measures, Mike said the COV-19 vaxxine took a weight off his dad’s shoulders.
“He was able to hang out with his friends. He was able to go to the grocery store and not wear a mask, see family members, and that’s really what ended up killing him was that he didn’t know the vaccine wouldn’t be effective for him,” said Mike Madry.
Daniel Madry ended up in the hospital around August 14 and died on August 24, Mike said. It was shocking to their family. Mike said his dad didn’t know he would still be so vulnerable.
“I really believe that if he had just one conversation, whether it be with a family member or his medical provider, that the vaccine may not be efficient for him, that he wouldn’t produce the antibodies, that there’s no question in my mind that he would have gone back to life the way before the vaccine came out,” Mike continued.
Now, Mike said he wants to share a message of caution with others like his dad to spare other families the grief they are experiencing.
“My hope is that somebody watching this who is immunocompromised like my dad and just didn’t know will really reevaluate their decision to not wear a mask and socially distance because if my dad did that he would still be here today. There’s no question,” he offered.
Mike said his dad got sick and went to the hospital around the same time the government-approved booster shots for immunocompromised people to help improve their immune response to the vaccine. He said he feels this also underscores how important it is for everyone to mask up, social distance and get vaccinated to protect themselves and others.
How Your Vaxxination Status Will Only Be Temporary
By Dr. Joseph Mercola
Data suggest 1 in 317 boys aged 16 to 17 will get myocarditis from the COVID shots, and after a third booster, that number may be even higher
VAERS reporting is likely underreported by a factor of 41. Since there are over 8,000 domestic deaths reported to VAERS, and 98% of those deaths are “excess deaths,” this suggests that as many as 300,000 Americans may have died from the COVID shots thus far
Calculations based on government data from 35% of the world’s population suggest we’re killing approximately 411 people per million doses on average. Moderna and Pfizer are both two-dose regimens, which pushes this to 822 deaths per million fully vaccinated. And that’s just the short-term mortality. We still have no concept of how these shots might impact mortality and morbidity in the longer term
An Italian investigation found that if the COVID mortality definition were changed to only include those cases where there were no preexisting comorbidities, the mortality from COVID comes out to just 2.9% of the overall reported number. This suggests that if a COVID death was redefined to being a death actually “from” COVID rather than “with” COVID, the death count could be substantially smaller than 760,000 deaths and may be smaller than the number killed by the vaccines
The deadliest vaccine ever made is the smallpox vaccine, which killed 1 in 1 million vaccinated people. The COVID shots kills 822 per million fully vaccinated, making it more than 800 times deadlier than the deadliest vaccine in human history
In this interview, Steve Kirsch, executive director of the COVID-19 Early Treatment Fund, reviews some of the COVID jab data he’s presented to the U.S. Food and Drug Administration and the Centers for Disease Control and Prevention during various meetings.
For example, during the September 17, 2021, FDA VRBPAC (Vaccines and Related Biological Products Advisory Committee) meeting,1 Kirsch cited data suggesting 1 in 317 boys aged 16 to 17 will get myocarditis from the shots, and after a third booster, that number may be even higher. He also cited data showing the Pfizer shot kills far more people than it saves. I’ll provide more details about that below.
Kirsch didn’t come into this due to some preconceived opinion about vaccines. He and his family have all received two doses of the COVID jab. It wasn’t until after the fact that he started hearing about problems from others that he started taking deep dives into the data. He explains:
“After I got vaccinated, a woman asked me, ‘Should I get vaccinated?’ And I said, ‘Of course, you should. This is the safest thing ever. Nobody’s died and there are no side effects. You’ve got to get this modern technology.’ I’m singing from the hymn book.
And then she said something that threw me off course because I said, ‘Why are you asking such a stupid question?’ And she said, ‘Well, three of my relatives got the vaccine and they died within a week.’ I said, ‘No, no, that can’t be true. There’s no way that can happen.’
I’m trying to convince her that she’s mistaken, that it must have been something else. I wrote her saying, ‘Statistically, you can’t have three people dying from the vaccine, which doesn’t kill anyone.’ And she wrote back and she said, ‘Yeah, but they’re dead.’
That was a game-changing moment for me … but I was still in denial … I was operating [from the position] that the FDA is still operating the same [conservative] way [they used to before], but they’re not … nor did I understand that the U.S. Centers for Disease Control and Prevention is now mission driven, and the mission is to get a needle in every arm. My trust was in the agencies.
The next incident involved my carpet cleaner, Tim Damroth. He showed up wearing a mask. And I’m saying, ‘Hey, you should all get vaccinated. Once you get vaccinated you don’t have to wear a mask.’ And he said, ‘Well, I did get vaccinated, but I had an extreme reaction. I had a heart attack two minutes after I got injected.’ He also described that his wife had [developed] Parkinson’s-like symptoms. Her left hand was shaking uncontrollably.”
The Price Truth-Tellers Pay
The data are ultimately what convinced him that people must be told the truth about these shots because, without that, they cannot give informed consent. He’s sacrificed a lot to do just that, including professional relationships and millions of dollars in lost income.
“I basically put my life on hold and started looking in the various databases and talking to people to understand what was going on,” Kirsch says. “And every place I looked, [the truth] became more clear to me. And so, on May 25, 2021, I wrote this 250-page article for TrialSiteNews. It may be the longest article for TrialSiteNews ever published.
When I wrote that article, within a week, every member of my [COVID-19 Early Treatment Fund’s] scientific advisory board quit — there were 14 scientists from all over the United States and in different fields with different expertise. They said I was ‘an evil person’ and that they never wanted to talk to me again in their life.
I pleaded with them, saying, ‘Look, if I’ve got the analysis wrong, then tell why can’t you tell me where I got it wrong.’ And they wouldn’t say anything. They just said, the vaccines are safe and I should be ashamed of myself.”
Kirsch also created and submitted a 177-page PDF slideshow to the October 26, 2021, VRBPAC hearing, titled, “Questions About the COVID Vaccine.”2 It’s an absolute treasure trove of information and I would encourage you to review this great resource that he is updating in real time.
VAERS Data Likely Off by Factor of 41
In his video, “Vaccine Secrets: COVID Crisis,”3 the first episode of “The False Narrative Takedown Series,” Kirsch explains how to estimate COVID jab mortality, which he and a team of statisticians have done based on a variety of sources, including but not limited to the U.S. Vaccine Adverse Events Reporting System (VAERS).
Kirsch estimates VAERS reporting is off by a factor of 41, and that anywhere from 150,000 to 300,000 Americans have died from the COVID shots.
“We looked at eight different ways and VAERS is just one of the ways. So, when people say, ‘You can’t use VAERS for this, you can’t [calculate] causality [based on VAERS data], I’m saying, ‘Fine. We got the same answer using seven other ways.
In the VAERS analysis, we determined that VAERS was under-reported by a factor of 41, which is quite reasonable … Ten years ago we had a system where we could actually discover all the unreported things in VAERS, and they discovered VAERS was severely underreported by as much as 95 times. Vaccines that we thought were safe, they’re not safe at all. So, what did they do? They killed the project.
So, the reason that we have such a bad system today is that it is intentional. If we had a good system, it would show all the flaws for all of these vaccines that we’ve been giving people.”
The system is clearly intentionally designed from a technical standpoint to radically decrease the number of cases entered. It takes more than 30 minutes to complete a single report and you can’t save it until completed, so if you walk away and get timed-out, you have to start all over.
Kirsch knows a neurologist in California who claims to have 2,000 COVID jab-injured patients (out of a client base of 20,000), but she’s only filed two reports to VAERS. She doesn’t have time for the rest. So, she’s under-reporting by a factor of 1,000. Also, while doctors are required by law to file adverse event reports, there’s no enforcement, and no punishment for not filing.
It is also important to note that no one is paid to enter this data. That could be a part time job for most clinicians, were they to responsibly report all the side effects and deaths.
COVID Shots Are Far Deadlier Than the Infection
Overall, his team’s calculations suggest we’re killing 411 people per million doses (and remember Moderna and Pfizer are both two-dose regimens), worldwide. And that’s just the short-term mortality. We still have no concept of how these shots might impact mortality in the longer term.
To put things into further perspective, October 21, 2021, an Italian investigation found that by changing the COVID mortality definition to only include cases where COVID-19 was the primary cause of death and there were no comorbidities decreased the death toll by 97%, from 130,000 to fewer than 4,000.
Kirsch believes the real death tally from COVID-19 in the U.S. may be about 50% of the reported number. This means about 380,000 Americans died from COVID-19 (rather than with COVID), whereas the COVID “vaccine” has killed as many as 300,000. In other words, it’s possible that the cure may be worse than the disease.
COVID Shot Is the Deadliest ‘Vaccine’ Ever Created
It gets even worse though. In Pfizer’s children’s trial, one of the participants, 12-year-old Maddie De Garay, suffered a number of devastating events, including paralysis. This side effect was misreported, however, and put down as “abdominal pain.” Neither the FDA nor the CDC has investigated the case, despite promising to do so. Pfizer has refused to investigate it as well.
In the youth trial, 1 out of 1,131 children was paralyzed. Meanwhile, Pfizer’s adult trial shows that the shot saves one COVID death for every 22,000 fully-vaccinated people. But for children, it’s estimated we need to fully vaccinate over 630,000 kids to save one life. That means we may permanently disable as many as 557 kids per life saved. Meanwhile, there’s not a single report of a healthy child dying from SARS-CoV-2 infection anywhere in the world.
This means the number needed to vaccinate to save one otherwise healthy child from COVID death is actually infinite, as they’re not dying from COVID to begin with. There simply is no doubt that in children, the COVID shot is no benefit and all risk. Kirsch notes:
“Dr. Paul Offit was interviewed 20 years ago on ‘CBS 60 Minutes,’ and he said the smallpox vaccine is so dangerous that we would never consider doing that in modern times. It’s the most dangerous vaccine ever invented … and the smallpox vaccines only kills one person per every million-people vaccinated, which is a lot.
You vaccinate 300 million people, you’re going to kill 300 people. That is unacceptable according to Offit, but he just voted for a vaccine that kills 822 people per million fully vaccinated [assuming a two-dose regimen].
That means these COVID vaccines are over 800 times deadlier than the deadliest vaccine in human history. So, this isn’t a close call. These vaccines are the deadliest vaccines ever created by man. And they’re promoted as safe and effective.”
COVID Shot Gets Deadlier the Younger You Are
Based on a request from Dr. Peter McCullough, Kirsch also analyzed COVID jab mortality based on age using the VAERS data. For 80-year-olds, he found we kill two people to save one. For 20-year-olds, we kill six to save one.
The younger you are, the greater the risk. The Kostoff analysis4 found this general pattern as well. Ronald N. Kostoff is a research affiliate in Gainesville, Virginia, who in 2016 wrote an expert review on under-reporting of adverse events in the biomedical literature.5
In a review published in October 2021, Kostoff found five elderly are killed by the shots for each elderly person saved, and the ratios get worse as you go down in age. That said, “the vaccines don’t make sense for any age group, which is exactly the same thing I found independently,” Kirsch says.
“Nobody should get these vaccines. There is no cost-benefit analysis that I have seen that shows it is beneficial … I mean, you’re not going to take an intervention that is just as likely to kill you as to save you.
You want to take an intervention which is at least 10 times more likely to save you than to kill you, because it’s an optional intervention. What kind of business do you have taking an intervention which has a marginal benefit for a completely unknown short- and long-term risk profile?
The other thing I want to say is that, the societal benefit argument, people are saying, ‘You’re selfish because you didn’t get vaccinated.’ Well, that’s irrational.
Have you ever seen a CDC analysis showing you the societal benefit of being vaccinated? It doesn’t exist. And there’s a reason it doesn’t exist, because the societal benefit would be so tiny that it’s ludicrous. Today, we know the vaccinated are as likely to spread the virus as the unvaccinated. So where is the societal benefit?
If there are no downsides [to the shot], then people would say, sure, maybe there’s some societal benefit. I’ll do that. But here your life is at stake and the data show that roughly 1 in 1,000 will get killed by these vaccines. So, if I say, hey, suppose sacrificing your life could save 100 person years (e.g., 10 people given another 10 years of life).
When I asked this live in a clubhouse room with a few hundred people, nobody raised their hand to volunteer to do that — to sacrifice their life to save 100 person years. And I said, ‘OK, what about 1,000 person years? If you could sacrifice your life to save people 1,000 person years, would you do it? Nobody would do that. It’s nonsensical.
We have a constitutional right to life … And I don’t think you’re being selfish about it. You have a family, you have friends, you have loved ones, you have people you interact with … Why would I ask you to sacrifice your life? To save people you don’t know?
Everybody has their own special way that they contribute to society. Why would we ever ask somebody to [sacrifice their life for a potential social benefit]? Maybe we should ask Joe Biden, ‘Joe, if you could give up your life to save 1,000 person-years, would you do that?’ It would be very interesting to see what he says.”
CDC Performs Statistical Magic, Again
Countering all of this data we have a recent CDC analysis,6 which concluded that people who get the COVID shot are two-thirds less likely to die of any cause.
“I sent Janet Woodcock my deck of 180 questions. I said, ‘Janet, I bet you can’t answer any of these 180 questions. Doesn’t this concern you?’ She sends back an email saying, ‘Look at the CDC analysis, showing that after you get the jab, there’s this two-thirds drop in mortality.’
My friends and I, when we saw in that paper, we were laughing our heads off over here. The stats on 18- to 44-year-olds [show] 35% die from accidents. The rest die from disease — cancer, heart disease, whatever.
The only way to get a two-thirds reduction [in all-cause mortality] is if nobody dies from anything anymore — any disease — and we also reduce the number of accidents that they have … This is the immortality drug. All kidding aside, there’s no mechanism of action that could possibly justify that people are going to be better off from a health perspective after getting these vaccinations. Zero.
Nothing is improved. You are not immortal. You are just the opposite; your immune system is compromised. You’re also more likely to get COVID. In the U.K., the government numbers show that 40-year-olds, after the honeymoon period is over, were more than twice as likely to get infected if they were vaccinated.
In the U.S., you have hospitals where you have a 50% community vaccination rate and the hospital admissions are 90% vaccinated people. You can’t make these statistics up.
In fact, the CDC was confronted by these statistics by Aaron Siri, who wrote about it on his substack, and they just ignored them. So, they make up stuff [and] this paper shows the CDC can put out anything and as long as it has that little CDC logo on it, people are going to believe it no matter how ridiculous it is.
And nobody in the medical community criticized it. I wrote a very popular article about it on my substack entitled, ‘FDA Discovers Fountain of Youth.’”
Biggest Fraud in History
All things considered, the COVID vaccination campaign is the biggest medical fraud in modern history. As Kirsch says, it’s a house of cards, held together by belief in data that aren’t there and avoidance of confronting the safety signals in the VAERS system and other studies that don’t comport with the narrative.
They even avoided the determination of one of the world’s top pathologists (Peter Schirmacher) that at least 30% to 40% of the deaths two weeks post-vaccine were caused by the vaccine. The still claim there are no deaths that have been attributed to the Pfizer or Moderna vaccines. That’s ridiculous.
“I’ve never seen anything like this, and I’ve never heard of anything like this because the conspirators who are telling this false narrative are all the three-letter agencies under the Department of Health and Human Services — the FDA, CDC and NIH.
They’re all in on it, Congress is all in on it, mainstream media’s all in on it, and the medical community is all in on it. They can’t afford to back down now because they are in it too deep. It would be too embarrassing to them.
We have been saying for months, ‘You guys have to look at the VAERS data,’ and they have been ignoring and censoring us rather than engaging us with dialogue — and none of these people will engage us in dialogue.
We tell the so-called ‘fact checkers’ where to look and what questions to ask the CDC to verify our stories and they never follow up. The ‘fact checkers’ all refuse to get on a recorded phone or Zoom call since they don’t want to be exposed as being biased.
One strategy for changing this is that we’re going to run a series of ads. Each of the ads will feature a unique personality, like a Dr. Peter McCullough, a sports figure, doctors, victims and so on. They’ll relate their personal anecdotes for what’s happened to them. And they will say, ‘Look, before you get vaccinated, check the facts. Listen to the other side of the story.’
It’s a reasonable ask. And we’ll direct them where to go to hear the side of the story that the mainstream media aren’t allowing them to hear. And then we let them make up their own mind. People aren’t hearing the other side of the story, and the White House is helping suppress it. When the White House has a hit list of censorship, it’s very clear what is going on. When in history have we done that?
Do you ever see McCullough on CNN? No, because they want to give you only one side and they’re deliberately giving you only one side of it, and they know it. If they want to give the impression they are balanced, they’ll pick someone who isn’t an expert and interview them. Robert Malone is never going to be on CNN. Malone invented the mRNA vaccine and yet he doesn’t qualify to talk about it on CNN?
America used to be a country that embraced a diversity of views, and you had freedom of speech, you had freedom to express your opinion. You had the freedom to tell the truth. No more. That freedom has been taken away.
If you don’t agree with the mainstream narrative, you’re silenced. And so, what we’re going to do is run the series of ads, and we’ll only be able to run it on alternate media because the mainstream media won’t run our ads because the ads encourage people to hear the other side of the issue.”
More Information
Again, you can download Kirsch’s 177-page PDF, jam-packed with questions and data on the COVID “vaccine.” I also urge you to review his “False Narrative Takedown” (TFNT) series, which you can find on his Rumble channel.
You can also peruse his website, skirsch.io, or follow him on his social media accounts, which include Twitter, Gab, Telegram and LinkedIn. To keep on top of his latest investigations, you can subscribe to his Substack channel. If you can afford it, consider signing up for a paid subscription. Select articles can also be found on TrialSiteNews.
“Substack is really important because they don’t censor people who tell the truth,” Kirsch says. “So, I really encourage people to support platforms like Substack. I also get a portion of that, and any money I get, I will donate 100% to funding ads and to fighting this. If we can get 100,000 subscribers at $5 a month, that’s $500,000 a month we can spend to combat false narrative. That’s serious fire power.
People ask me, why am I doing this? I’m not making any money off of this. I have no conflicts of interest. I have no history as a conspiracy theorist or spreader of misinformation. We’ve lost all our friends.I was forced out of my job because I wanted to speak out against the vaccines.
I’m losing money on this because I’m funding a lot of the things out of my personal pocketbook. The donors that donated to the early treatment fund, none of them, not a single one, is supporting the effort to get the truth out about how dangerous these vaccines are and how wrong the mandates are.
My motivation is a 100% on saving lives. That’s my reward in life. If I can save one life, my life was worth living. If I can save 100 lives, even better. If I can save 100,000 lives, that is more meaningful than anything I’ve ever done or will do.”
Mahima Mathew: 31-Year-Old Pregnant Woman Dead 10 Days After Covishield (AstraZeneca) Injection
By The COVID Blog
Ms. Mahima Mathew
PALA, KERALA — A 31-year-old pregnant woman is dead after a doctor’s orders to accept her own slaughter.
Ms. Mahima Mathew received the first experimental Covishield viral vector DNA injection on August 6, according to the Kerala Kaumudi. Covishield and Vaxzevria are two other brand names for the AstraZeneca injections, similar to Comirnaty and Pfizer. A Pala gynecologist recommended she receive the injection despite also learning she was seven weeks pregnant that day.
Five days later, on August 11, Ms. Mathew suffered debilitating headaches. She went back to the same Pala hospital that day. Doctors gave her pain killers and antacids before sending her home. Ms. Mathew was back in the hospital on August 15 when her condition worsened. She was declared brain dead the next day and officially deceased on August 20.
A post-death examination revealed Ms. Mathew suffered from a brain hemorrhage. Her death certificate says she “may have” died as a result of the AstraZeneca injection. The news was exacerbated by two more women’s deaths after experimental injections that week. Ms. Divya Nair received her first Covishield/AstraZeneca injection on August 2. The 38-year-old suffered brain bleeding and died on August 22.
A 21-year-old woman called Renjitha of Vavadukkam received her first Covishield/AstraZeneca injection on August 3. She developed blood clots in her brain and died on August 25.
James Cooper Sawyer: 77-Year-Old Fealthy Tennessee Father and Grandfather Gets Third mRNA Booster Shot, Dead Eight Days Later
By The COVID Blog
Mr. Jim Sawyer
COOKEVILLE, TENNESSEE — An active 77-year-old father and grandfather was warned by his daughter not to get a booster shot. He’s now dead and the daughter is warning others to avoid the boosters.
Mr. James “Jim” Cooper Sawyer received a third Pfizer mRNA “booster shot” on August 20, according to his daughter Leah Flaga. Pfizer booster injections are currently recommended by the Centers for Disease Control (CDC) only for immunocompromised people. Thus it is unclear why or how Mr. Sawyer even got the third injection, as he was described as healthy and vibrant by his family. The CDC reported that one million Americans have received booster shots as of August 31.
Mr. Sawyer immediately started “not feeling right” after the third injection. He text-messaged his daughter that day, asking her if she could help explain the adverse effects he was experiencing. No more information is provided thereafter. Mr. Sawyer passed away “suddenly and unexpectedly” on August 28.